fetching data ... 
Background: Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAV) are a group of rare autoimmune diseases characterized by inflammation of small-sized blood vessels and associated with the presence of ANCA that target the autoantigens proteinase 3 (PR3) and myeloperoxidase (MPO) in neutrophils. ANCA are considered the main pathogenic drivers of vasculitis in AAV, and they have been extensively described [1]. In this context, ANCA-producing B cells play a central role in AAV pathogenesis [2], but information on B cell receptor (BCR) isotypes of autoreactive B cells in AAV is sparse.
Objectives: The aim of this work is to characterize circulating autoreactive PR3-specific B cells (PR3+ B cells) by studying IgG, IgA and IgM BCR isotypes in AAV patients and healthy donors (HD) and to explore potential associations with immunological status, disease activity and treatment groups.
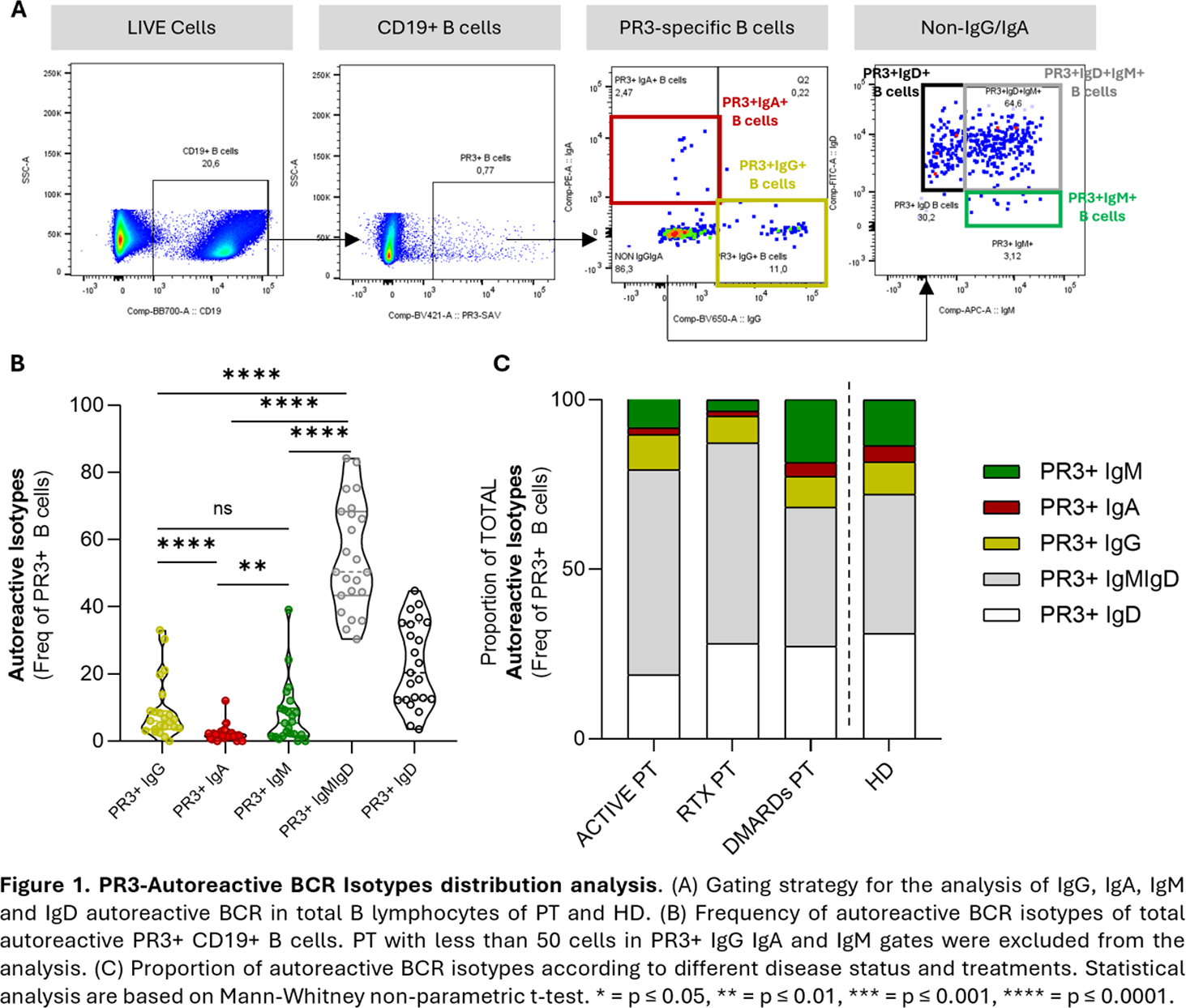
Methods: Peripheral blood mononuclear cells (PBMCs) from PR3-ANCA+AAV (PR3-AAV) patients (either granulomatosis with polyangiitis (GPA),or microscopic polyangiitis (MPA)) and HD were collected and analysed by conventional flow cytometry. A customized 11-color panel for surface markers was used to detect circulating PR3+ B cells, using biotinylated,conformationally intact, human recombinant inactive PR3 [3] and streptavidin-BV421 to detect anti-PR3 BCRs. A live/dead staining was included to monitor cell viability. 1x10 6 PBMCs were incubated with anti-CD19-RB705; anti-IgD-FITC; anti-CD27-BV786; anti-CD38-BV510; anti-CD24-PE-Cy7 and specific anti-IgG-BV650, anti-IgA-PE, anti-IgM-APC antibodies to detect BCR isotypes. B cells and autoreactive subpopulations were analysed by the expression of lineage markers ( Figure.1A ). Clinical data and outcomes were collected from clinical charts and were correlated with PR3+ B cells (total and subsets). Serum levels of IgG, IgA and IgM PR3-ANCA were measured by ELISA.
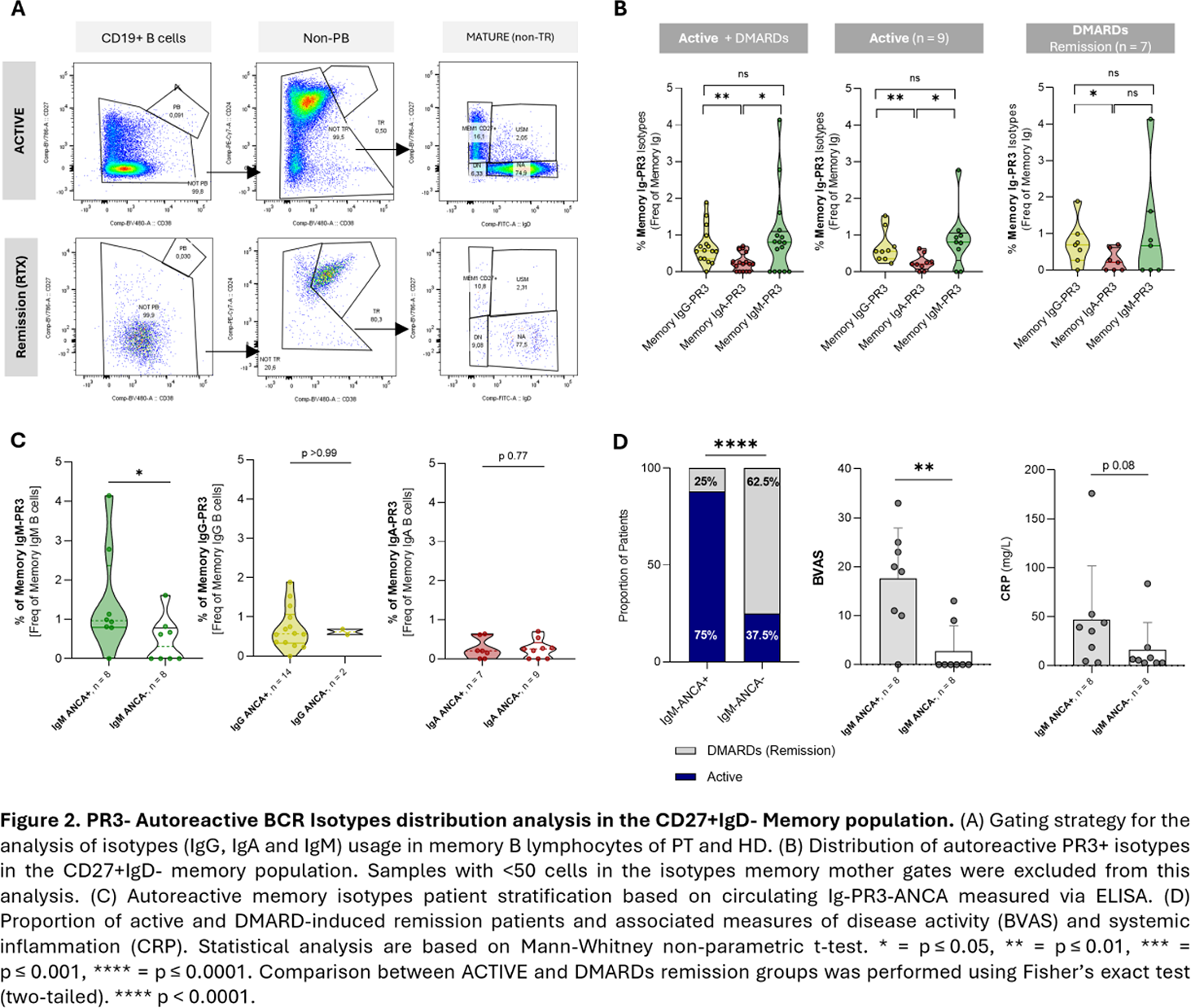
Results: This study was performed on a cohort of 30 PR3-AAV patients (87% GPA [n=26]; 13% MPA [n=4]) and 10 HD. The median age of PR3-AAV patients was 65.5 years (IQR: 48.75-74.25) with 30% female, similar to HD (66.5 years, IQR: 52.75-76.25; 40% female). PR3-AAV were classified according to disease status into patients with active disease (n=11, 9 GPA, 2 MPA), patients in clinical remission on methotrexate, azathioprine or mycophenolate mofetil (DMARDs, n=7, all GPA), and patients in clinical remission after rituximab treatment (RTX, n=12, 10 GPA, 2 MPA). Peripheral blood samples from patients were collected after B-cell repopulation (CD19+ ≥10 cells/mL). All rituximab-treated patients were off rituximab for at least 6 months at the time of sampling. The analysis of the autoreactive PR3+ B cell pool revealed an enrichment of PR3+ B cells in the IgD+IgM+ compartment as compared to other isotypes in the whole group of patients ( Figure.1B ; 50.4% (IQR: 43.4-68.4), p<0.0001 for all comparisons). In all patients, the autoreactive PR3+IgG+ B cells (6.05%, (IQR: 3.51-8.96)) and PR3+IgM+ B cells (5.34%, (IQR: 1.57-9.82)) were expanded compared to PR3+IgA+ B cells (1.66%, (IQR: 0.85-2.33); p<0.0001 and p=0.0028, respectively). When comparing autoreactive PR3+ B cells in different disease and treatment groups, patients in remission on DMARDs and HD had a similar distribution of Ig subsets, while patients with active disease and in remission induced with RTX differed significantly ( Figure.1C ). In RTX treated patients, the landscape of autoreactive BCR isotypes was dominated by IgD+IgM+. All groups had similar proportions of IgG and IgA; IgM were expanded in patients in remission with DMARDs (10.63%, IQR: 8.8-32.3) and active patients (4.6%, IQR: 1.9-15; p=0.12 between these 2 groups) compared to patients in remission induced with RTX (1.8%, IQR: 0.3-6.7; p=0.03). Next, we analysed the memory compartment (CD24+CD38+CD27+IgD-), given its relevance in immunological memory and potential disease reactivation. RTX-treated patients were excluded from this analysis as B-cell repopulation after RTX resulted in insufficient cells within the memory gate (explanatory images in Figure.2A ). When looking at the PR3+ B cell proportion in IgG-, IgA-,and IgM-memory B cell compartments, PR3+IgG+ (0.58%, IQR: 0.36-0.98) and PR3+IgM+ (0.81%, IQR: 0.0-1.37) isotypes were more abundant than PR3+IgA+ (0.21%, IQR: 0.0-0.44; p=0.0018 and p=0.029, respectively; Figure.2B ). The stratification of patients based on positivity to different isotypes of serum PR3-ANCA revealed that patients positive for IgM PR3-ANCA have expanded PR3+IgM+ memory B cell population compared to patients negative for IgM PR3-ANCA (p=0.0468). This was not observed when stratifying the patients based on serum IgG PR3-ANCA and IgA PR3-ANCA positivity (p>0.99 and p=0.77, respectively) ( Figure.2C ), suggesting a correlation between autoreactive memory B cell expansion and serum autoantigen-specific IgM. Finally, patients positive for serum IgM PR3-ANCA showed significant associations with disease activity, as assessed by Birmingham Vasculitis Activity Score (BVAS), and systemic inflammation, as assessed by C-reactive protein (CRP, Figure.2D ).
Conclusions: Overall, our findings indicate that the PR3-specific B cell pool was enriched in the IgD+IgM+ compartment, particularly marked in patients in remission induced with RTX. The autoreactive IgM+ compartment was more expanded in active patients and patients in remission on DMARDs as compared to RTX-treated patients, suggesting a consistent breach of self-reactive clones from central tolerance. When focusing on the autoreactive memory compartment, PR3-AAV patients exhibited an enriched autoreactive IgM fraction, correlating with serum IgM PR3-ANCA. The stratification by serum IgM PR3-ANCA was also associated with disease activity and systemic inflammation; these results inform our understanding and further investigations of the role of antigen-specific IgM in disease pathogenesis and patient stratification.
REFERENCES: [1] Kitching et al., Nat Rev Dis Primers, 2020.
[2] Berti et al., JCI Insight, 2021.
[3] Silva et al., J Autoimmun, 2010.
Acknowledgments: NIL.
Disclosure of Interests: None declared.