fetching data ... 
Background: Behçet’s Disease (BD) is a chronic vasculitis characterized by painful mucocutaneous lesions that impair quality of life. Apremilast, a selective phosphodiesterase-4 (PDE4) inhibitor, has demonstrated efficacy in BD-related oral ulcers (OUs) in clinical trials and real-world studies [1-3]. While apremilast has been reported to inhibit neutrophil activation in BS [4], its effects on other immune cells remain unclear. Based on our preliminary findings [3], this study further investigates the molecular mechanisms of apremilast using both transcriptomic analysis and immunological experimental validation, with a specific focus on its action on monocytes.
Objectives: To elucidate the molecular mechanisms using integrated transcriptomic analyses, with a focus on the role of the transcriptional regulator BACH1 in monocyte-driven inflammation and oxidative stress.
Methods: Bulk RNA sequencing was performed on peripheral blood mononuclear cells (PBMCs) from complete or partial responders (N=15) at baseline and after 3 months of apremilast treatment. HC monocytes were treated with or without apremilast before LPS stimulation to model BD inflammation in vitro, and were subsequently analyzed by transcriptomic sequencing. BD and HC-derived monocyte assays evaluated cytokine expression, reactive oxygen species (ROS) production, and superoxide dismutase (SOD) activity in response to apremilast. Transcription factors (TFs) and target genes were predicted using ChEA3, and TF-target correlations were calculated (Pearson r > 0.8). Gene network modules were identified using the MCODE algorithm in Cytoscape. BACH1’s role was explored via transcriptomic network analysis and siRNA knockdown validation.
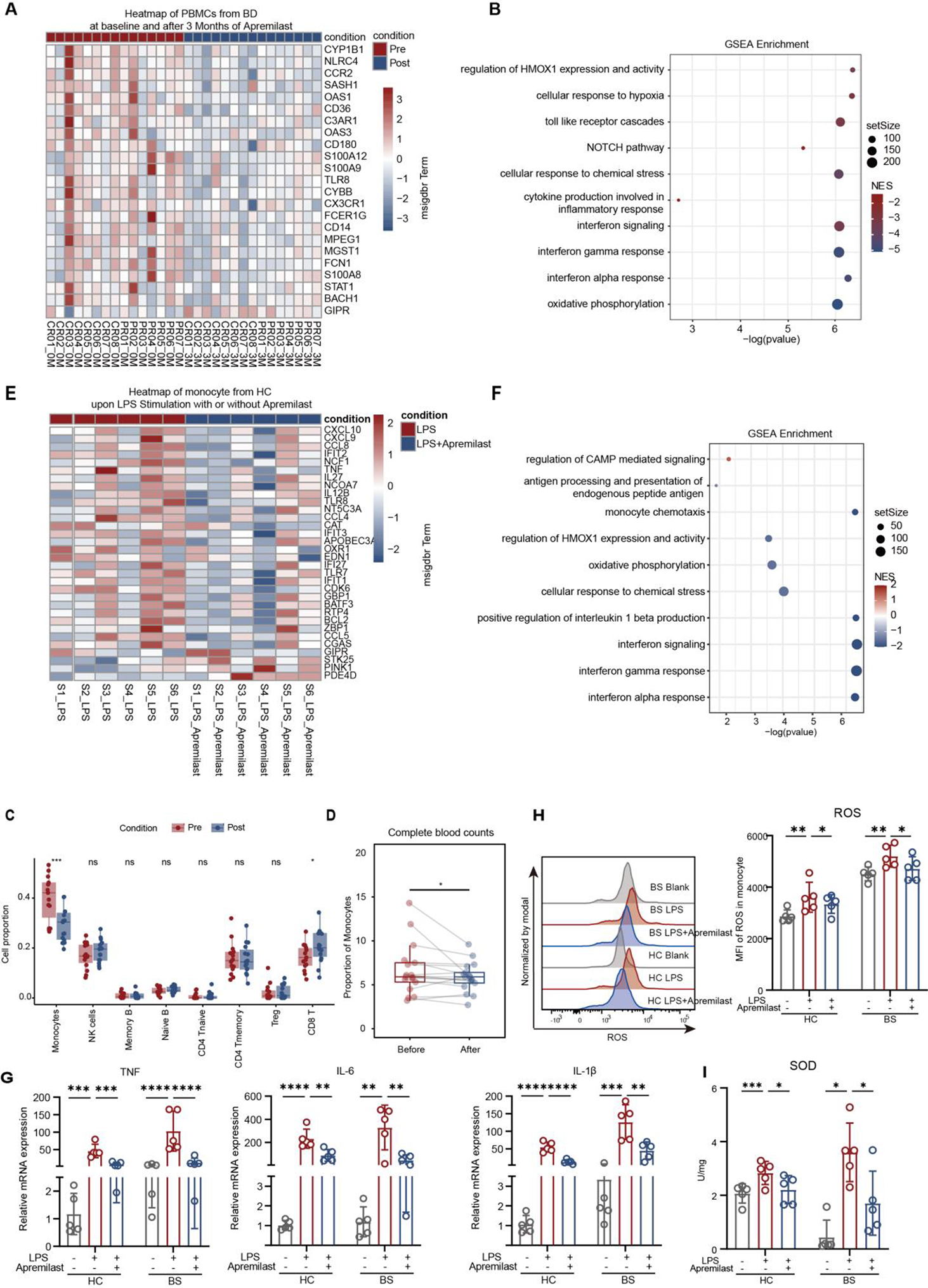
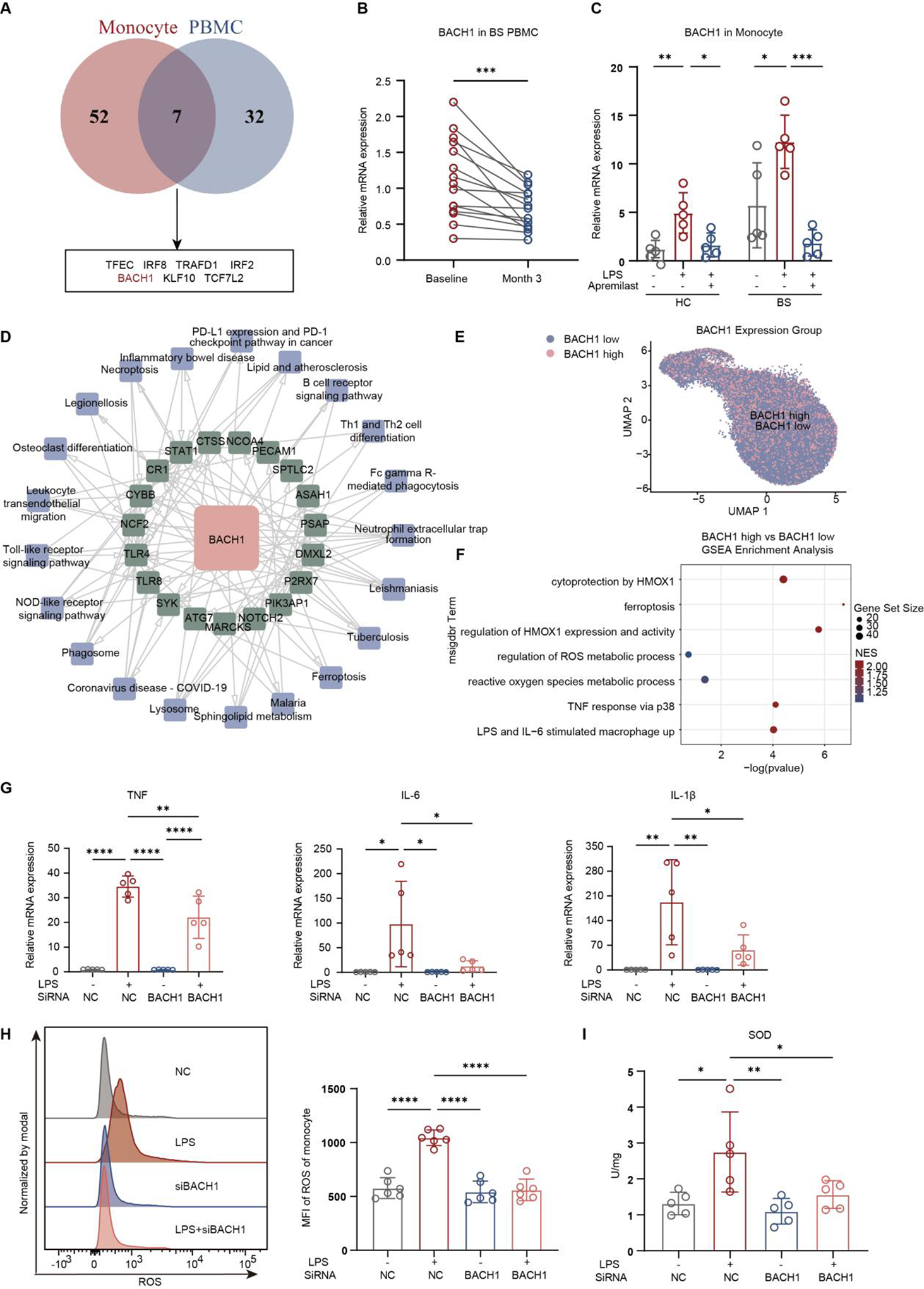
Results: Transcriptomic analysis of PBMCs revealed that apremilast significantly suppressed interferon signaling, oxidative stress, and cytokine/chemokine pathways (Figure. 1A-B). Notably, apremilast reduced the proportion of circulating monocytes, as shown by CIBERSORT deconvolution (39.1% ± 10.2% to 27.4% ± 7.2%, p < 0.001; Figure. 1C) and complete blood counts (6.7% ± 3.0% to 5.9% ± 1.7%, p < 0.05; Figure. 1D). The in vitro monocyte model recapitulated the transcriptional suppression of inflammatory and oxidative stress pathways observed in patient PBMCs (Figure. 2E-F). In vitro, apremilast attenuated LPS-induced inflammatory and oxidative responses in both BD and HC monocytes, significantly reducing TNF-α, IL-6, and IL-1β expression (p < 0.05, Figure. 2G), suppressing ROS accumulation (p < 0.05, Figure. 2H), and restoring SOD activity (p < 0.05; Figure. 2I). Integrative transcriptomic analysis identified BACH1 as a central downregulated transcription factor in both clinical PBMCs and in vitro monocytes (Figure. 2A-C). BACH1 expression was enriched in proinflammatory monocytes from BD patients and correlated with inflammatory and oxidative stress pathways (Figure. 2D-F). Functionally, siRNA-mediated BACH1 knockdown in monocytes recapitulated apremilast’s effects, reducing proinflammatory cytokine expression, lowering ROS levels, and enhancing SOD activity (Figure. 2G-I).
Conclusions: Apremilast improves refractory OUs in BD patients by suppressing monocyte-driven inflammation and oxidative stress via BACH1 downregulation. These findings provide novel insights into the cell-specific immunomodulatory mechanism of apremilast, identifying BACH1 as a key molecular mediator and offering a new potential therapeutic target for BD.
Integrated transcriptomic and functional validation of the effects of Apremilast on PBMCs and monocytes in BD
( A )Heatmap of DEGs between baseline and Month 3 of BD patients (N = 15). ( B ) Dotplot of selected enriched pathways modulated by apremilast in GSEA analysis results. ( C ) CIBERSORT deconvolution showed decreased monocyte proportions in PBMCs. ( D ) Monocyte proportions in BD patients before and after 3 months of apremilast, based on complete blood counts (N = 17). ( E ) Heatmap of DEGs between monocytes stimulated with LPS and LPS plus apremilast. ( F ) Dotplot of selected enriched pathways modulated by apremilast in monocytes in GSEA. ( G-I ) TNF-α, IL-6, and IL-1β expression ( G ), intracellular ROS levels ( H ), and SOD activity ( I ) in apremilast-pretreated monocytes derived from BD patients and HCs measured after LPS-stimulation.
BACH1 is a central regulator of monocyte inflammation and oxidative stress and mediates the anti-inflammatory effects of apremilast.
( A ) Venn diagram showing 7 overlapping downregulated TF in both PBMCs from apremilast-treated BD patients and in vitro monocytes cultured with apremilast. ( B ) BACH1 expression in BD PBMCs at baseline and 3 months (N = 15). ( C ) BACH1 expression in apremilast pretreated monocytes derived from BD patients and HCs was measured after LPS-stimulation. ( D ) Protein-protein interaction (PPI) network identifies BACH1 as a central hub among apremilast-regulated genes in PBMC from apremilast-treated BD patients. ( E ) UMAP plot of previously published monocyte scRNA-seq data, stratified into BACH1-high and BACH1-low (≤ 0) subsets. ( F ) GSEA of BACH1-high versus BACH1-low monocytes. ( F-H ) TNF-α, IL-6, and IL-1β expression ( G ), intracellular ROS levels ( H ), and SOD activity ( I ) in BACH1-silenced monocytes measured after LPS-stimulation.
REFERENCES: [1] Hatemi G. et al. Apremilast for oral ulcers associated with active Behçet’s syndrome over 68 weeks: long-term results from a phase 3 randomised clinical trial. Clin Exp Rheumatol. 2021; 39 Suppl 132, 80–87.
[2] Hirahara L. et al. Efficacy and safety of apremilast for 3 months in Behçet’s disease: A prospective observational study. Mod Rheumatol. 2021; 31(4), 856–861.
[3] Liu Y, Wang X, Liu J, Chen H, Zheng W. Apremilast in the treatment of refractory mucosal Behçet’s syndrome and its potential molecular mechanisms. EULAR 2023; POS0333.
[4] Le Joncour A, et al. Reduction of Neutrophil Activation by Phosphodiesterase 4 Blockade in Behçet’s Disease. Arthritis Rheumatol. 2023;75(9):1628-1637.
Acknowledgments: NIL.
Disclosure of Interests: None declared.