fetching data ... 
Background: Metatarsophalangeal (MTP) 1 joint is the predilection site for monosodium urate crystal depositions in gout, which may induce both flares with a high degree of inflammation and lead to erosive damage in the joint. Imaging with Dual Energy CT has shown an association between tophi and erosions in several joints. Ultrasound is sensitive for assessing crystal depositions, and the Outcome Measure in Rheumatology (OMERACT) ultrasound group has defined three ultrasound elementary lesions of crystal depositions in gout: tophi, double contour, and aggregates. Further, ultrasound has been shown to be sensitive for the detection of erosions. However, knowledge about gout-related erosions is limited, especially regarding associations between the severity of ultrasound detected crystal depositions and the presence of erosions.
Objectives: To explore the associations between the degree of ultrasound detected elementary lesions of crystal depositions and presence of erosions in MTP1 joints in patients with gout.
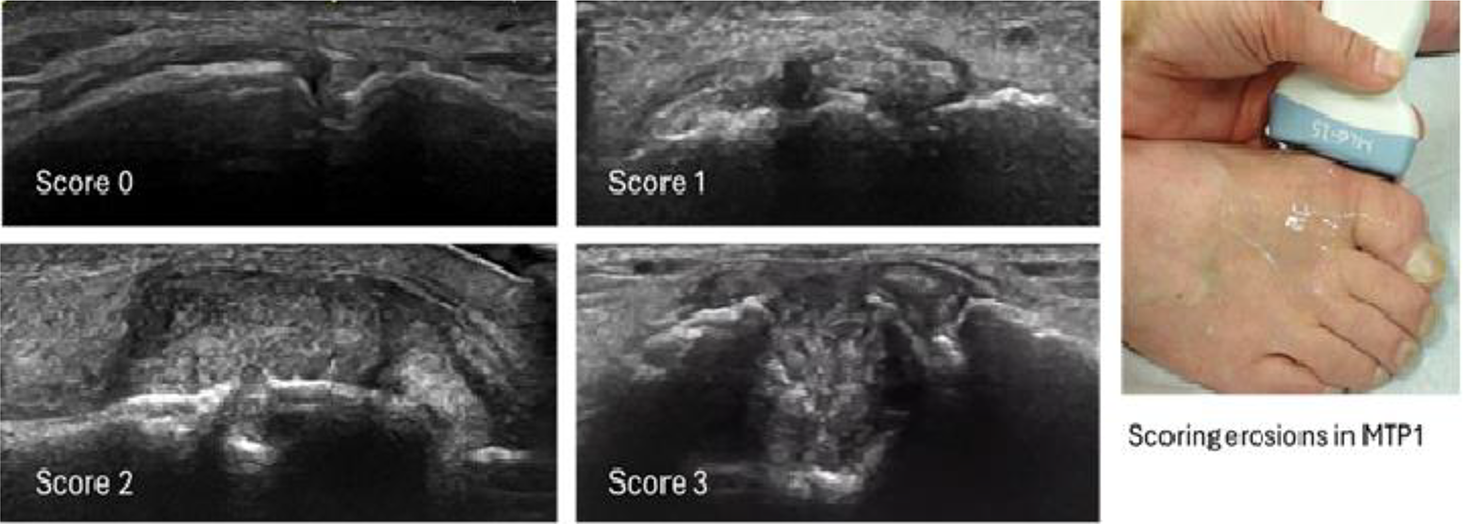
Methods: The established NOR-Gout study is a longitudinal study with treat-to-target urate lowering therapy (ULT) of gout patients examined by clinical, laboratory (including serum urate), and ultrasound assessments (bilateral examination of radiocarpal, 2 nd metacarpophalangeal joints, knee, ankle, and 1 st metatarsophalangeal joints as well as triceps, quadriceps, patellar (proximal and distal) and Achilles tendons) at baseline and after 1, 2 and 5 years. Ultrasound of the MTP1 joints included dorsal and medial assessments for tophi, double contour and aggregates, scored according to the OMERACT scoring system (0=none, 1=uncertain, 2=definite and 3=major). Erosions were assessed at the dorsal and medial head of the first metatarsus using similar scoring system as for depositions (figure 1), reflecting the size of the erosion, and with the presence of an erosion defined as score 2 or 3. Statistics included independent samples t-test (for exploring differences in variables dependent on presence of erosion) and paired samples t-test (for exploring changes between visits).
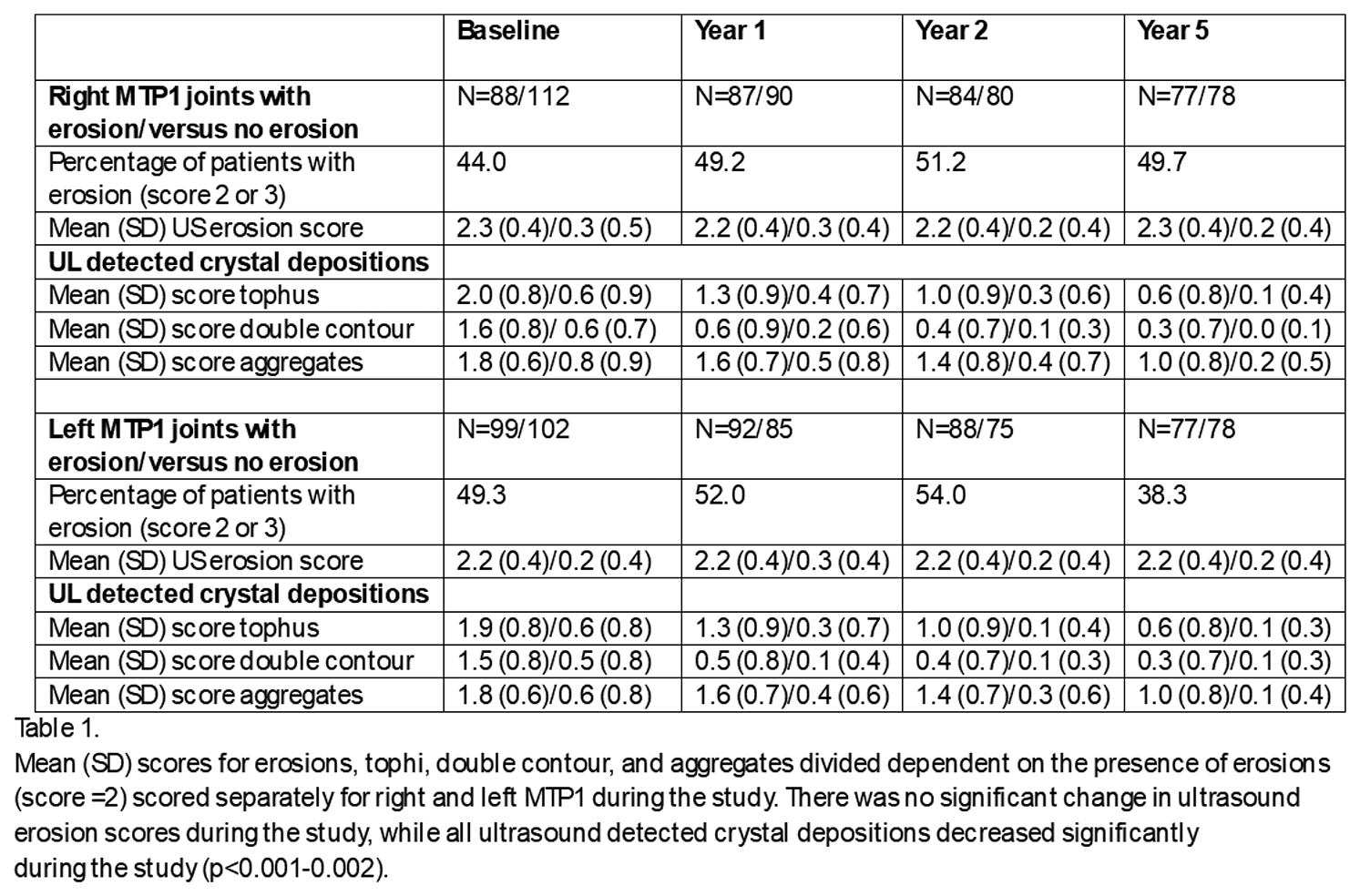
Results: From the NOR-Gout study [1], 201 patients had assessments of erosions and were included (95.5% men, mean (SD) age 56.4 (13.7) years, time since first flare 7.9 (7.7) years). All patients were prescribed ULT, and the mean (SD) serum uric acid (µmol/L) decreased during the study from 499 (77) at baseline, to 311 (49) at 1 year, 322 (66) at 2 years and 337 (84) at 5 years. Presence of MTP1 erosions at either right or left side was 46.6% at baseline (score 0=39.7%, score 1=13.7%, score 2=36.9%, score 3=9.7%), with no significant changes during the 5 years. Higher total sum scores of elementary lesions from all examined locations, higher age and longer disease duration were all associated with presence of MTP1 erosion (p<0.001 for all). The mean (SD) ultrasound scores of crystal depositions in MTP1 joints (bilaterally) decreased from baseline to 5 years; 1.2 (1.1) to 0.3 (0.6) for tophi, 1.0 (0.9) to 0.2 (0.5) for double contour, and 1.2 (0.9) to 0.6 (0.8) for aggregates (p<0.001 for all). Table 1 shows the highly significant differences in the scores of elementary lesions in the MTP1 joints depending on presence or absences of erosions (p<0.001-0.002), and there was a continuously decrease in crystal depositions, independent of presence of erosion.
Conclusions: This study showed a close association between presence of erosion in MTP1 and the severity of crystal depositions in the same joint, with similar finding for all the three elementary lesions. During the study with treat-to-target ULT, the crystal depositions in MTP1 joints showed a major decrease, while the erosion score did not change significantly. Our study supports the concept that local crystal depositions respond to ULT, while erosions did not change over the five years study. However, importantly, there were no further deterioration of erosions. Thus, ULT is important for elimination of crystal depositions as well as inhibiting erosive progression.
REFERENCES: [1] Hammer HB, Karoliussen L, Terslev L, Haavardsholm EA, Uhlig T. Ultrasound-detected crystal depositions and clinical flares dissolve during successful urate-lowering therapy: 5-year follow-up results from the treat-to-target NOR-Gout study. Ann Rheum Dis. 2025 Nov 20:S0003-4967(25)04517-0. doi: 10.1016/j.ard.2025.10.029.
Acknowledgments: NIL.
Disclosure of Interests: Hilde Berner Hammer AbbVie, UCB, Novartis, Lars Fridtjof Karoliussen: None declared, Lene Terslev Novartis, Roche, BMS, Pfizer, Espen A. Haavardsholm Novartis, Janssen-Cilag, and AbbVie, Till Uhlig Galapagos, Pfizer, and UCB.