fetching data ... 
Background: There is a growing body of investigative literature suggesting that one or more fibromyalgia (FM) plasma constituents, most likely IgG, are neurotoxic, particularly to the Dorsal Root Ganglia (DRG). This toxicity has been demonstrated in human-to-murine passive transfer models involving native FM subjects and those sustaining FM after COVID-19 infection. The mechanism for this injury pattern is thought to be via irritative IgG binding to the dorsal root ganglia (DRG) complex, and particularly to satellite glia cells (SGC). Nevertheless, the specificity and contextual importance of IgG binding to the DRG in FM remains the subject of investigation, as such binding has also been observed in other autoimmune disorders (e.g., rheumatoid arthritis). Therefore, we asked whether this IgG binding of the DRG might be part of a wider spread IgG-tissue deposition which could be diffusely injurious to neural tissue in FM and even more injurious to delicate DRG structures. In other words, might FM be a systemic disorder whose painful manifestations are augmented or amplified by anti-DRG binding? We sought to investigate this question by studying the murine distribution properties of IgG infused from a subset of FM subjects with EMG/ nerve conduction studies (NCS) demonstrating evidence of Chronic Inflammatory Demyelinating Polyneuropathy (CIDP).
Objectives: We used PET/CT scanning to track the body wide distribution of IgG infused from FM patients with CIDP (FM - CIDP) in a murine model. We sought to determine if enhanced IgG deposition might be more widespread than previously thought.
Methods: All FM - CIDP subjects were voluntary participants in a companion study utilizing plasmapheresis (PLEX) in recalcitrant FM. The details of their demographics and the clinical outcome of their PLEX therapy are to be communicated in a separate report. In brief, FM subjects were assessed clinically by a rheumatologist with a special interest in FM (XJC, SM). Eight subjects [6 female, mean age 54 yrs (range 29-75 yrs)] meeting ACR 1990 FM criteria resistant to all standard treatments, gave informed consent for PLEX therapy and subsequent plasma harvesting (COH IRB # 204333). Inclusion criteria required subjects to undergo an EMG/ NCS, carried out by a single electromyographer (JDM), who conducted a 4 extremity NCS (22 total nerves) and one-sided arm and leg needle EMG. Each participant met EAN/PNS 2021 electrodiagnostic criteria for CIDP; all were also examined by our neurologist (NP). All subjects had the general-medical and cardiovascular reserve to withstand PLEX. Patients with any other known cause of peripheral neuropathy, including diabetes mellitus (Hb A1c > 6.5), were excluded. Adequate peripheral or central venous access was also a prerequisite to participation. FM-CIDP subjects underwent five sessions of plasmapheresis, 1 - 3 liters each, carried out over ≤ 8 days. FM-CIDP IgG was purified over immobilized Protein G [2]. Female, 8–10-week-old C57Bl/6 mice were injected IP with saline or 8 mg of commercial IVIg or 8 mg of FM-CIDP IgG and then PET/CT imaged with 64 Cu-DOTA-goat anti-human IgG (100 µCi, 10 µg) one week post injection. PET/CT imaging (Molecubes; Lexington, MA. USA) was performed at 4h, 24h, and 48h post injection; tissue samples were collected from mice euthanized at 48 h.
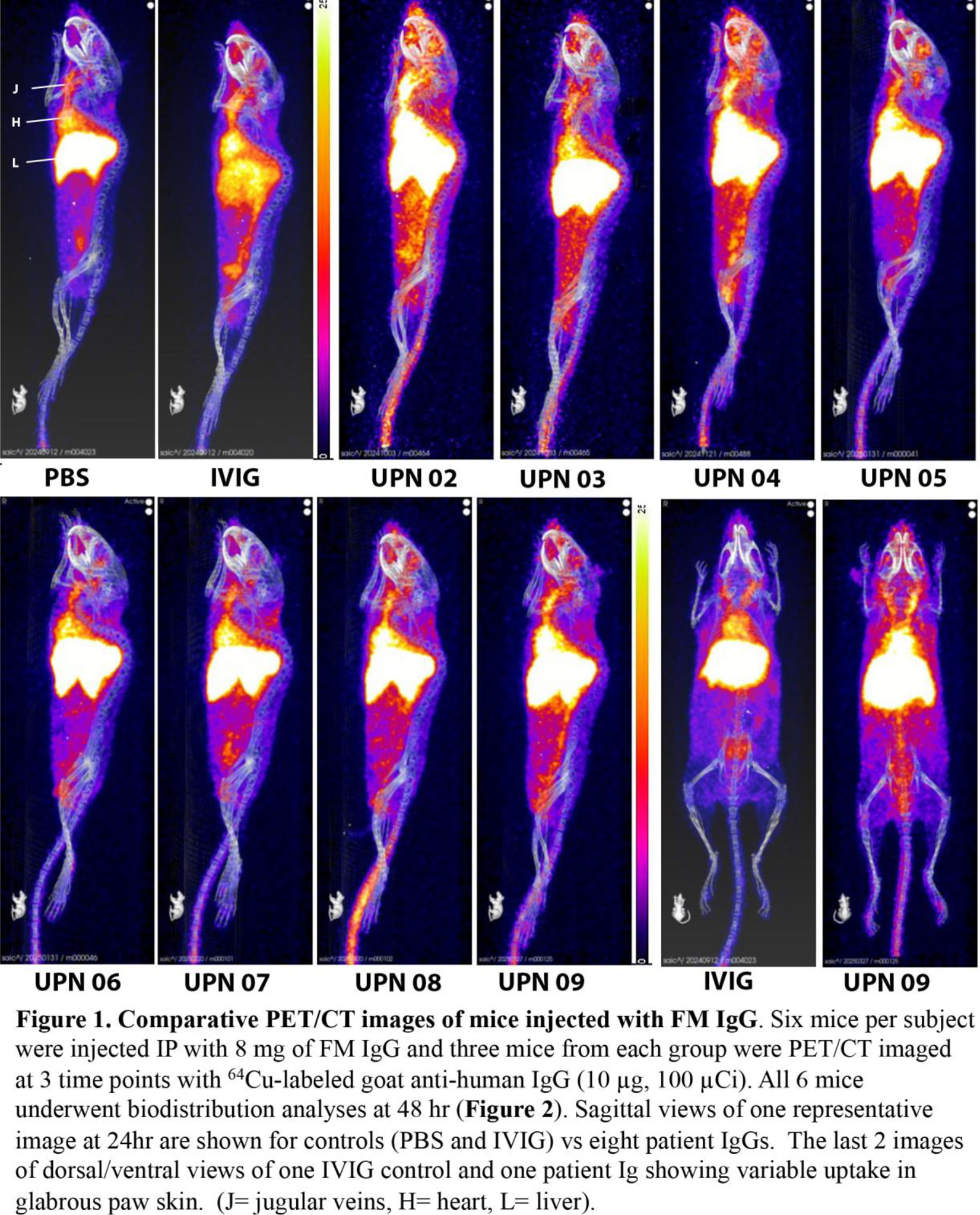
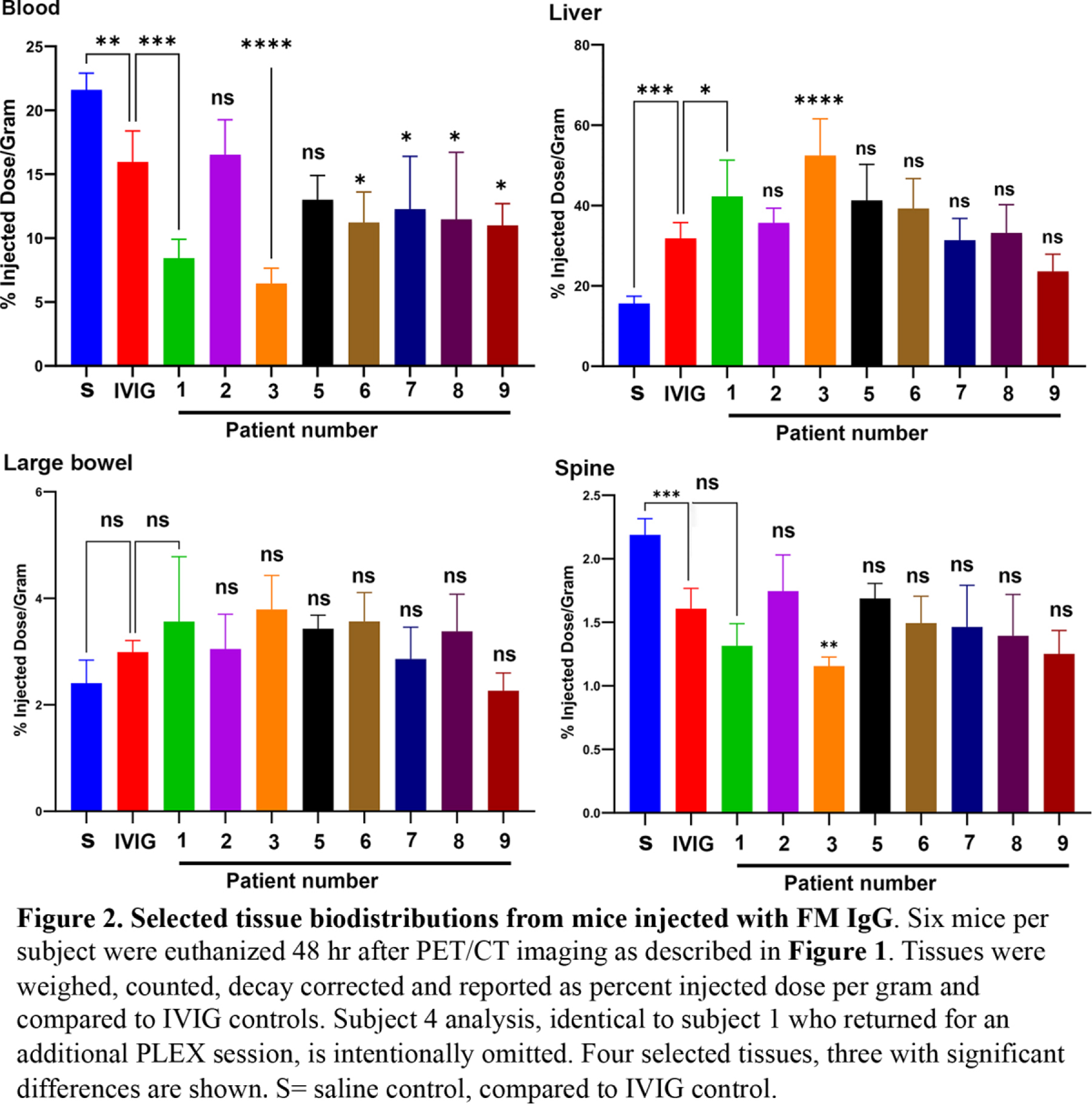
Results: Serial IgG yield analyses in one FM-CIDP subject’s 5 PLEX series demonstrated an exponential decay curve, with removal of ≈70% total circulating IgG after 5 PLEX sessions. The 24hr PET/CT imaging results for saline controls showed expected tracer retention in the blood (heart and venous flow) and liver, while the commercial IVIg controls had decreased blood and increased liver retention. In contrast, the FM-CIDP IgG groups showed increased blood tracer clearance and widespread residual tracer uptake in whole body images (Figure 1). Blood tracer clearance in 6 of 8 FM-CIDP IgG treated mice was significantly greater than commercial IVIg controls while having generally similar biodistribution of tracer to liver, large bowel, and spine (Figure 2). Although skin and spine uptake were uniformly low by tissue counting, there was evidence of localized FM-CIDP IgG uptake in hind paw skin and various vertebrae by PET/CT (Figure 1). Goat anti-human IgG tissue staining of hind paw skin exhibited local FM-CIDP IgG uptake with simultaneous decreased epidermal nerve fiber density (i.e., small fiber neuropathy).
Conclusions: The results of our PET/ CT scan study show that mice injected with FM-CIDP IgG demonstrate significantly more rapid blood tracer clearance of their IgG compared to controls. This rapid clearance is accompanied by increased, diffuse whole-body tracer uptake of FM-CIDP IgG compared to commercial IVIg controls. It is suggested, therefore, that IgG tissue deposition in FM likely represents a systemic phenomenon rather than one confined to paraspinal areas, such as the DRG alone. We reason that this finding is due to whole-body enhanced vascular permeability (EVP), probably due to a subtle systemic inflammatory disorder. It seems reasonable to speculate that substance(s) leading to this EVP allow soft tissue ingress of noxious substance(s) to access DRG and other peripheral neural tissues. This injury pattern could lead to molecular changs in the DRG complex and resultant autoimmunity directed against altered molecular structures within the DRG. The final message to be derived from these data is that successful treatment of FM may require systemic immunotherapy, rather than that directed against anti-SGC antibodies alone. Clearly, further investigation is warranted.
REFERENCES: [1] Goebel A, et al. Passive transfer of fibromyalgia symptoms from patients to mice. J Clin Invest 202.
[2] Sensi, S, et al. Human Auto-IgG Purification from High Volume Serum Sample by Protein G Affinity Purification. Bio Protoc 2022.
[3] Caro XJ, et al. Evidence of peripheral large nerve involvement in fibromyalgia. Eur J Rheumatol 2018.
Acknowledgments: NIL.
Disclosure of Interests: None declared.