fetching data ... 
Background: Methotrexate (MTX) is a common therapy for patients with inflammatory rheumatic diseases (iRMD). In Germany, metamizole ist frequently prescribed as an effective and well tolerated pain medication. Combined metamizole and MTX use substiantially increases risk of severe agranulocytosis and should be avoided, especially in people aged ≥ 80 years [1,2].
Objectives: To analyse trends in the frequency of and risk groups for metamizole prescriptions in MTX-treated patients with iRMD.
Methods: Adults diagnosed with ≥ 2 ICD-10 codes of an iRMD and and prescribed MTX were identified from Barmer health insurance data covering 15.9 million persons from 2006 to 2024. Rheumatoid arthritis (RA), Psoriatic arthritis (PsA), axial Spondyloarthritis (axSpA), Polymyalgia rheumatica/giant cell arteritis (PMR/GCA), connective tissue diseases (CTD) and vasculitides were eligible. Concomitant prescriptions of metamizole, nonsteroidal antirheumatic drugs (NSAIDs), opioids, glucocorticoids (GC) and biologic disease modifying antirheumatic drugs (bDMARDs) were identified by Anatomical Therapeutic Chemical (ATC)-codes and described by age groups and and calendar years. Cumulative doses in 2024 were calculated using defined daily doses (DDD) as issued by the World Health Organisation. Comorbidities were assessed by Elixhauser Score. Odds ratios (OR) for metamizole use were calculated by a logistic regression model with opioid/GC/NSAID/bDMARD prescription (yes/no), sex (male/female), and age as independent variables. Agranulocytosis cases within 90 days after overlapping prescriptions of MTX and metamizole were identified using ICD-10-German modification codes D70, D61.1, D61.8, D61.9.
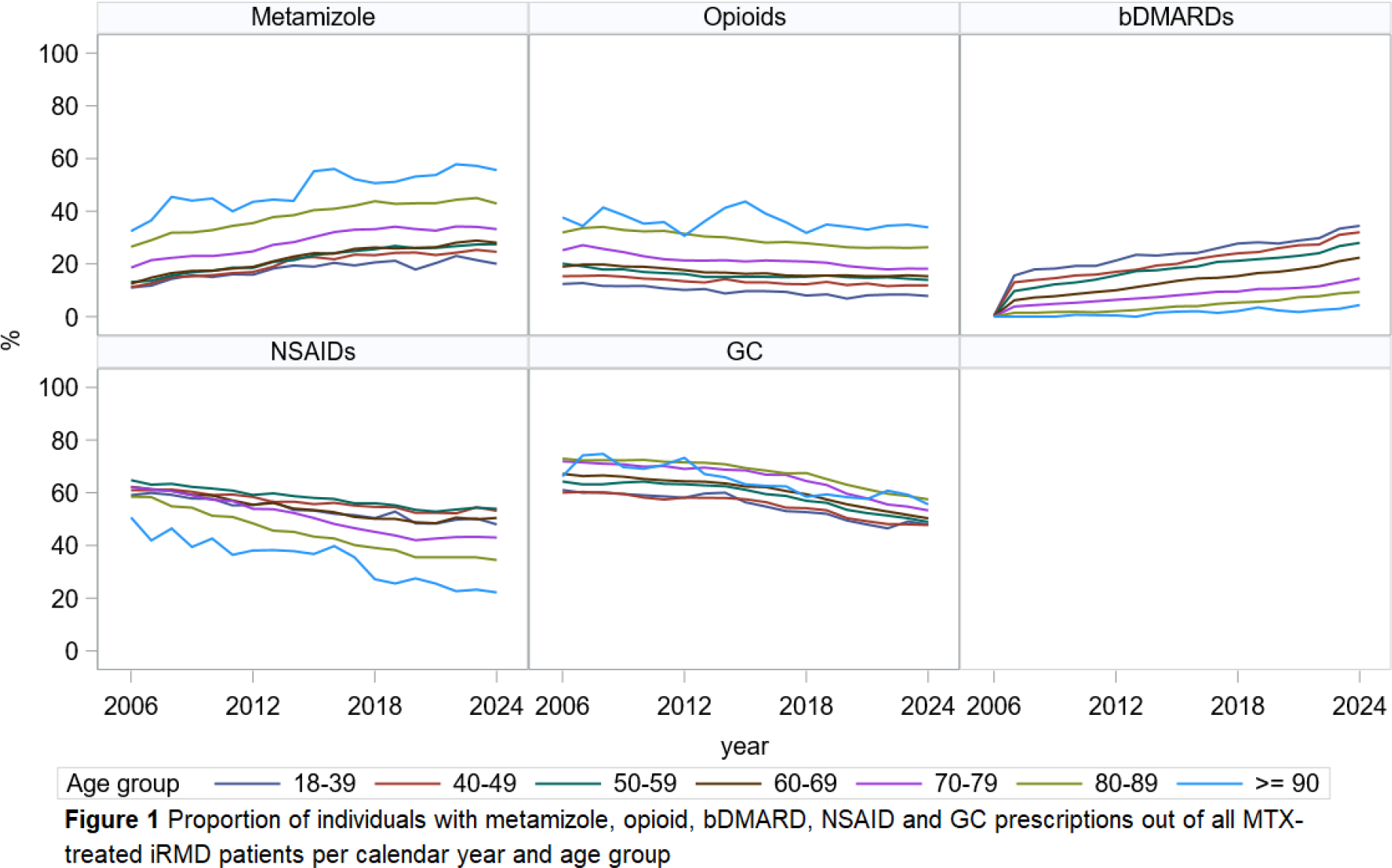
Results: Between 28,160 (2006) and 49,859 (2024) patients with an iRMD and MTX therapy were observed. In 2024, 52% had a diagnosis of RA, 16% PsA, 13% PMR/GCA, 13% CTD, 4% axSpA and 2% vasculitides. Osteoarthritis (38%), liver disease (20%), cardiovascular disease (17%) and cancer (14%) were common comorbidities in 2024 MTX users. Metamizole was prescribed to 32% of MTX users in 2024, the 50,090 prescriptions were provided mainly by general practitioners (73%), orthopedists (10%), other specialists (10%) and rheumatologists (8%). Metamziole prescriptions increased from 15% in 2006 to 32% in 2024 while prescriptions of NSAIDs (62% to 46%), GC (66% to 52%) and opioids (20% to 18%) decreased. Prescription of bDMARDs rose from 0.2% in 2006 to 20% in 2024. People ≥ 80 years were most often prescribed metamizole, opioids and GC, while younger persons were more likely to receive NSAIDs and bDMARDs (figure 1). Cumulative metamizole dose (DDD) in those with a metamizole prescription increased by age while cumulative NSAID doses decreased (table 1). In Opioids, GC and bDMARDs the cumulative doses did not change with age- only the proportion of patients using it. The odds for using metamizole was higher for patients with a prescription of opioids (OR metamizol prescription in opioid use vs. no use 3.6 [3.4; 3.8]), GC (OR vs. no use 1.6 [1.5;1.6]), NSAIDs (OR vs. no use 1.4 [1.4;1.5]), bDMARDs (OR vs. no use 1.1 [1.0;1.2], female sex (OR women vs. men 1.3 [1.2;1.3]) and older age (OR per 10 years 1.2 [1.2;1.3]) in 2024. Compared to RA, metamizole was prescribed more frequently for all other iRMD, especially for axSpA (OR 1.2 [1.1; 1.4]). There were 55,855 patients with overlapping prescriptions of MTX and metamizole at some time in the observation period. -Of those, 407 patients were hospitalised for agranulocytosis within 90 days. Agranulocytosis cases per 10,000 persons were 73 for all ages, 34 for 18-39 years, 11 for 40-49 years, 20 for 50-59 years, 54 for 60-69 years, 91 for 70-79 years, 189 for 80-89 years and 263 for ≥90 year olds.
Conclusions: Metamizole is being prescribed at an increasing rate, particularly in the high-risk group of MTX-treated iRMD patients ≥ 80 years. This goes along with an increased use in patients with a GC, NSAID and/or opioid prescription. Hospitalisations for agranulocytosis after overlapping use of MTX and metamizole were markedly increased in patients 70 years and older. Adequate DMARD therapy in the elderly and interdisciplinary information about the risk of agranulocytosis is needed to reach all groups of physicians involved in the care of patients with iRMD.
Prescriptions in 2024 in MTX-treated persons with iRMD. Medication use shows % of users and DDD (defined daily doses) among those with a prescription.
| Total | 18-39 | 40-49 | 50-59 | 60-69 | 70-79 | 80-89 | ≥90 years | |
|---|---|---|---|---|---|---|---|---|
| N | 49,859 | 1,685 | 3,123 | 8,357 | 14,473 | 12,901 | 8,730 | 590 |
| Female, % | 72 | 69 | 72 | 71 | 70 | 72 | 75 | 75 |
| Elixhauser, mean (SD) | 4.1 (2.5) | 2.1 (1.5) | 2.7 (1.8) | 3.2 (2.1) | 3.9 (2.3) | 4.7 (2.5) | 5.3 (2.6) | 5.4 (2.5) |
| Metamizole, % | 34 | 21 | 26 | 29 | 30 | 35 | 46 | 59 |
| mean cumulative DDD | 28 | 18 | 22 | 23 | 26 | 29 | 35 | 42 |
| Opioids, % | 19 | 8.3 | 13 | 15 | 16 | 19 | 28 | 36 |
| mean cumulative DDD | 116 | 117 | 118 | 137 | 124 | 108 | 119 | 116 |
| GC, % | 55 | 51 | 51 | 52 | 53 | 57 | 61 | 59 |
| mean cumulative DDD | 149 | 157 | 148 | 150 | 149 | 152 | 144 | 154 |
| NSAIDs, % | 49 | 51 | 56 | 57 | 54 | 46 | 37 | 23 |
| mean cumulative DDD * | 118 | 107 | 129 | 132 | 125 | 107 | 99 | 87 |
| bDMARDs, % | 19 | 37 | 33 | 28 | 22 | 14 | 8.2 | 3.6 |
| mean cumulative DDD | 267 | 256 | 274 | 272 | 272 | 261 | 244 | 264 |
* A cumulative DDD for GC of 149 (all ages) is equivalent to a daily prednisolone dose of 4mg.
REFERENCES: [1] Hoffmann et al. Agranulocytosis attributed to metamizole: An analysis of spontaneous reports in EudraVigilance 1985-2017. Basic Clin Pharmacol Toxicol 2020;126:116-125.
[2] Fiehn C et al. Assessment of interactions and dosage recommendations of synthetic DMARDs. Evidence-based and consensus-based recommendations based on a systematic literature search. Z Rheumatol 2024;83(Suppl 1):8-19. doi:10.1007/s00393-022-01308-z.
Acknowledgments: NIL.
Disclosure of Interests: Johanna Callhoff Janssen, Idorsia, Pfizer, Falk Hoffmann: None declared, Christoph Fiehn Medac, Medac, Ursula Marschall: None declared, Katinka Albrecht: None declared.