fetching data ... 
Background: Somatic mutations in hematopoietic stem and progenitors cells have recently emerged as key contributors to systemic autoinflammation, as illustrated by the description of the VEXAS syndrome. Chronic myelomonocytic leukemia (CMML) is a clonal myeloid disorder characterized by monocytosis and harboring recurrent somatic driver mutations. Severe VEXAS-like systemic autoimmune or autoinflammatory diseases (SAID) without UBA1 mutation are observed in up to 20% of CMML patients and are classically refractory to conventional immunosuppressive strategies. The mechanisms underlying these manifestations remain poorly understood.
Objectives: We hypothesized that specific recurrent somatic mutations driving CMML pathogenesis may underlie concomitant inflammation leading to SAID emergence.
Methods: We performed unbiased mutation enrichment analysis in 285 CMML patients, comparing patients with SAID (SAID+) to those without SAID (SAID–). We then performed genotype–phenotype correlation analyses stratified on mutational status, assessing SAID phenotype and inflammatory response to various treatment strategies including bDMARDs and clone-targeted therapies. Exploratory analyses were performed in a subset of CMML SAID+ patients to identify cell types and inflammatory pathways implicated in SAID pathogenesis.
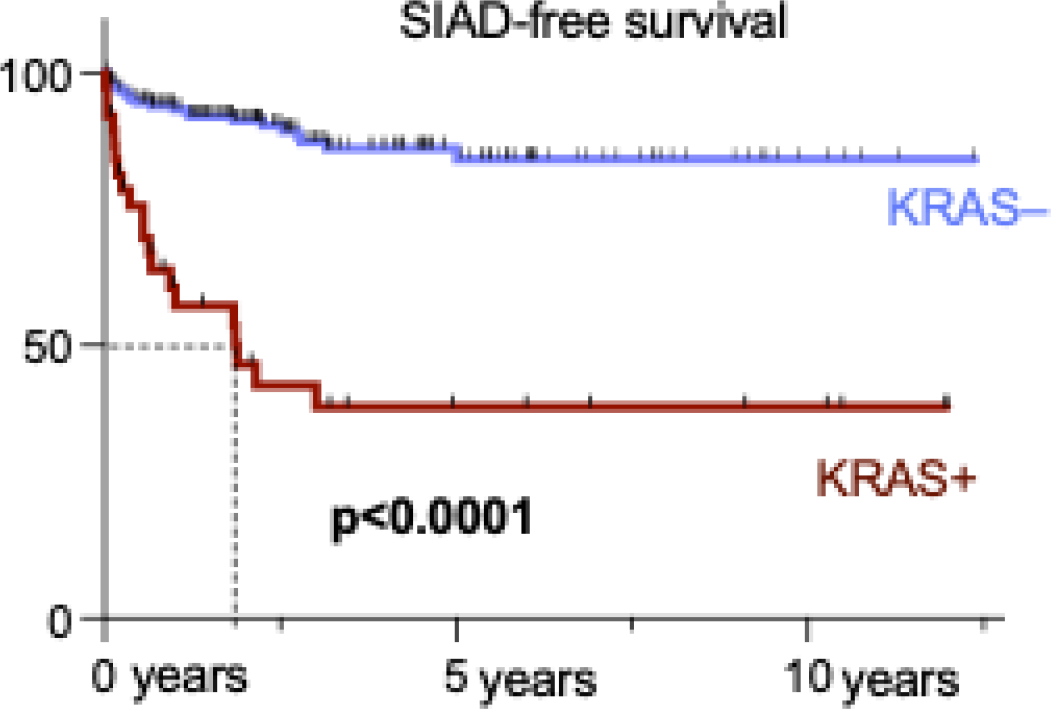
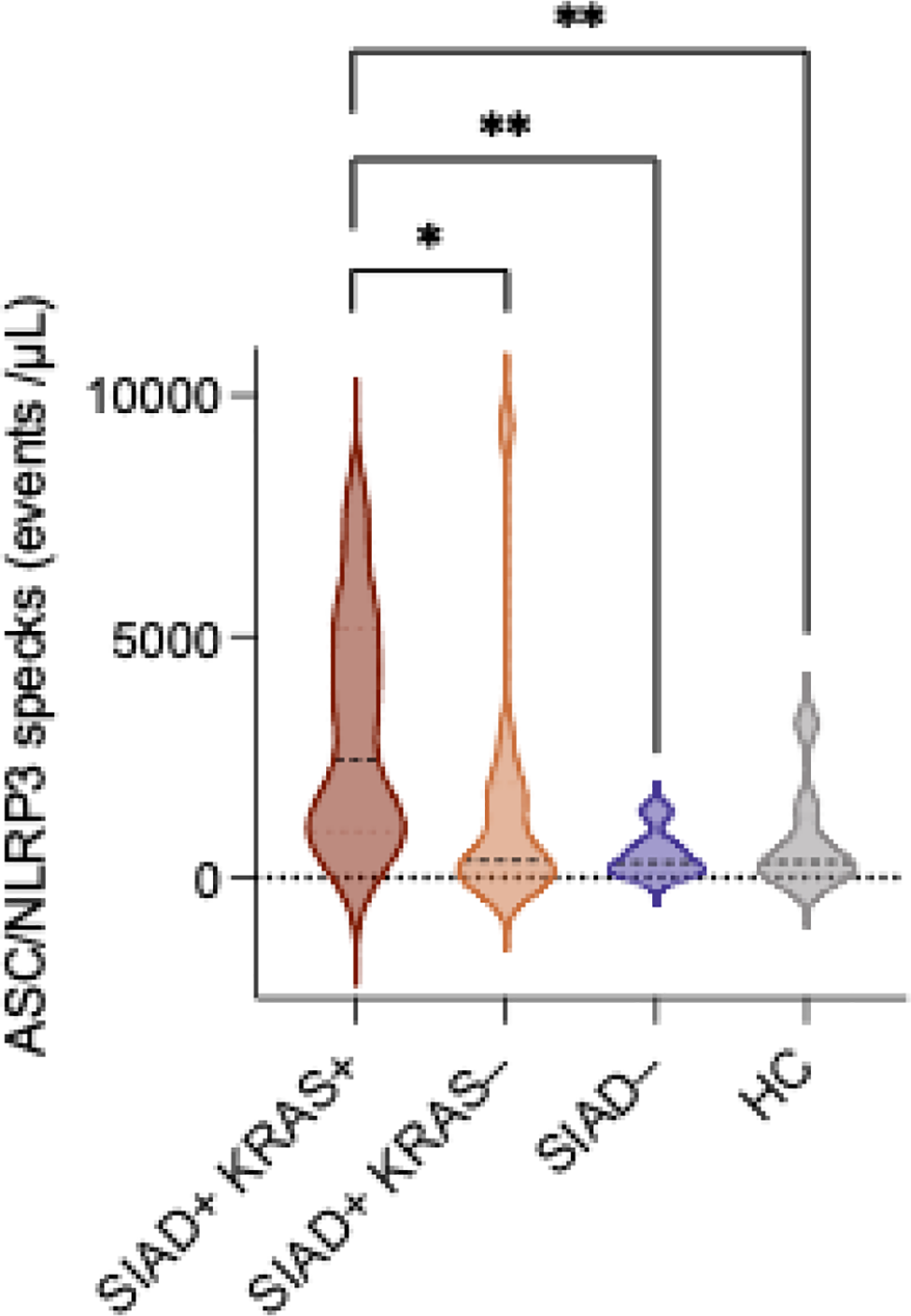
Results: Among 285 CMML patients, 91 (32%) had concomitant SAID. Patients from the CMML SAID+ group showed a higher prevalence of mutations in genes involved in the RAS/MAPK pathway compared with CMML SAID– patients (54% vs 39%, p=0.02), primarily driven by an enrichment in KRAS mutations (36% vs 9%, p<0.0001). Prevalence of SAID was significantly higher in KRAS -mutated (KRAS+) CMML patients compared to KRAS unmutated (KRAS–) patients (64% vs 25%, p<0.0001) (image 1). KRAS variants identified in SAID+ patients were predominantly gain-of-function mutations located at the p.Gly12 position, restricted to monocytes and dominant over other CMML driver mutations. Of note, 6 of 8 patients (75%) harboring single somatic KRAS mutations exhibited inflammatory manifestations. Additionally, somatic KRAS mutations were identified in 6 patients (2%) from a cohort of 265 UBA1 -negative individuals with VEXAS-like SAID, including two patients without overt hematological malignancy, further supporting a specific role of KRAS as a driver of autoinflammation. SAID+ KRAS+ patients displayed a distinct inflammatory phenotype compared to SAID+ patients without KRAS mutation, with high prevalence of serositis (52%), lymphadenopathy (36%), xanthelasma (18%) and aortitis (12%). SAID+ KRAS+ patients also showed elevated levels of serum ASC/NLRP3 specks (image 2) combined with high concentrations of IL-1β and IL-1RA, suggesting an implication of the NLRP3 inflammasome pathway. SAID associated with KRAS mutations were frequently steroid-dependent and poorly responsive to bDMARDS and clone-targeted treatment by hypomethylating agents (18% and 0% complete response rates at 12 months, respectively). One SAID+ KRAS+ patient treated with anakinra achieved complete inflammatory remission sustained at 24 months. Two SAID+ KRAS+ patients were treated with MEK inhibitors targeting RAS/MAPK signaling and achieved complete inflammatory remission.
Conclusions: Together, our results suggest that somatic KRAS mutations could act as a driver of myeloid-associated autoinflammation. Patients harboring these mutations often exhibit severe, treatment-refractory SAID, potentially driven by NLRP3 inflammasome activation in KRAS -mutated monocytes. These findings support targeted therapeutic approaches directed against IL-1 signaling or the RAS/MAPK pathway in a subset of VEXAS-like SAID patients.
SAID-free survival according to KRAS mutational status
Measurement of serum ASC/NLRP3 specks by flow cytometry according to presence of SAID and KRAS mutational status
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.