fetching data ... 
Background: Adult-onset Still’s disease (AOSD) exhibits marked clinical heterogeneity, yet no validated framework exists to classify patients based on underlying inflammatory biology or to inform cytokine-targeted therapy. In this study, we prospectively and retrospectively analyzed cytokine profiles, peripheral immune-cell phenotypes, and hepatic immune infiltration using a multi-platform approach integrating serum cytokine clustering, flow cytometry, Imaging Mass Cytometry, and histopathology.This study offers a mechanistic basis for cytokine-guided stratification and brings forward a precision-medicine framework with direct therapeutic implications for AOSD.
Objectives: To identify cytokine-based endotypes of adult-onset Still’s disease (AOSD) and explore their immunological characteristics and clinical implications for biologic selection.
Methods: Serum levels of 12 cytokines were measured in 144 patients with AOSD and 33 healthy controls (HCs). Correlations among cytokines, disease activity, and in-depth immune subsets were analyzed. Unsupervised clustering and t-SNE visualization were applied to define cytokine endotypes, which were validated in an independent prospective AOSD cohort (n=124) using a k-nearest neighbor algorithm and stepwise ROC-derived cut-offs. Flow cytometric analysis of T- and B-cell subsets in depth was conducted simultaneously with cytokine measurements across endotypes. Using Imaging Mass Cytometry (IMC), we concurrently generated a comprehensive immune-cell landscape of the affected liver tissue and validated the infiltration patterns of different immune subsets by immunohistochemistry (IHC).
Results: AOSD patients showed significantly elevated IL-1β, IL2, IL-6, IL-8, IL-10, IFNα, and IFNγ compared with healthy controls (HCs) (all p<0.05). Cytokine networks were highly interconnected and closely associated with disease activity. Three distinct cytokine endotypes were identified: an IL1β-dominant endotype, a hyperinflammatory (IL-6/IL-8/IFNγ-high) endotype, and a hypo-inflammatory endotype with relatively lower cytokine levels compared to the other clusters but still elevated versus HCs. The hyperinflammatory endotype exhibited higher Pouchot scores and macrophage activation syndrome frequency than the other groups (all p<0.05). Validation in the prospective cohort reproduced the three endotypes, and combination therapies targeting distinct inflammatory cytokines markedly reduced the length of hospitalization. Comprehensive immunophenotyping identified predominant CD4 + /CD8 + central memory T cells in the IL-1β–dominant endotype, whereas the hyperinflammatory endotype showed marked T-cell activation (CD8 + TEMRA, HLA-DR + CD3 + ) with elevated IFNγ. Corresponding hepatic tissue exhibited pronounced infiltration of activated CD8 + T cells and abundant neutrophils.
Conclusions: Cytokine profiling identifies immunologically distinct AOSD endotypes linked to disease severity, providing a rationale for cytokine-guided stratification and personalized biologic therapy.
Cytokine-based clustering and cross-cohort Validation in AOSD
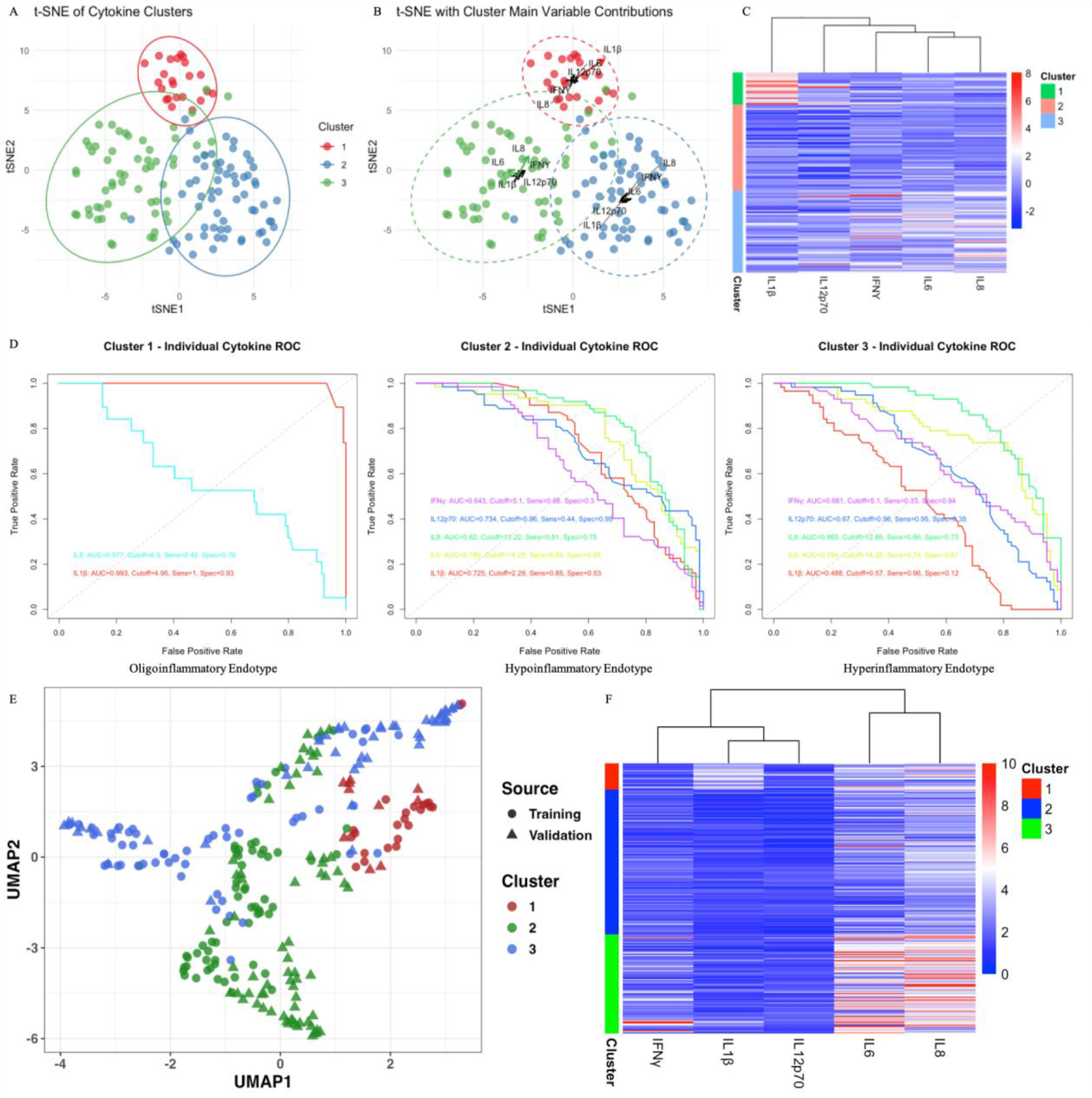
1. t-SNE embedding based on cytokine profiles shows that AOSD patients can be stratified into three distinct clusters; B. Cluster centroid vectors highlight the dominant contributing cytokines for each group, with IL-1β driving Cluster 1, IL-6/IL-8 driving Cluster 2, and IL-6/IL-8/IFN-γ driving Cluster 3; C. Heatmap depicts the standardized expression patterns of individual cytokines across patients, illustrating inter-cluster differences in inflammatory profiles; D. Stepwise ROC curves were generated for each AOSD cluster based on five circulating cytokines (IL-1β, IL-6, IL-8, IL-12p70, IFN-γ). Distinct cytokine patterns define three AOSD clusters, with key discriminatory cytokines and ROC metrics annotated in each panel; E. UMAP of training and validation cohort patients based on five serum cytokines mentioned in Figure 2D. Points represent individual patients, colored by cluster (1–3) and shaped by cohort. F. Heatmap of z-score–normalized cytokine expression in the validation cohort. Color intensity indicates relative expression (blue = low, white = median, red = high).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.