fetching data ... 
Background: Variants in the NOD2 gene are associated with increased susceptibility to a broad spectrum of diseases, ranging from granulomatous conditions (e.g. Crohn’s disease, Blau syndrome) to autoinflammatory disorders, such as Yao syndrome. These variants may variably affect NOD2 protein function, depending on the specific mutation, resulting in altered innate immune signaling and dysregulated inflammatory responses upon microbial stimulation. In recent years, targeted next-Generation Sequencing (NGS) gene panels have become a cornerstone of molecular diagnostic, enabling confirmation or diagnostic support for genetically heterogeneous disorders, including adult-onset conditions associated with NOD2 variants.
Objectives: This study aimed to identify amongst adult patients with autoinflammatory manifestation, such as recurrent fever, skin rashes, and gastrointestinal symptoms, those who present NOD2 variants. Additionally, we sought to explore whether specific NOD2 variants correlate with distinct clinical phenotypes, potentially allowing the reclassification of adult patients from the nonspecific “undifferentiated autoinflammatory disease” (uSAID) into potential emerging subgroups of NOD2-related disorders. These conditions span a phenotypic continuum encompassing granulomatous diseases, intestinal pathologies, and autoinflammatory disorders.
Methods: Patients with clinical and biochemical features suggestive of autoinflammatory disease and referred to the outpatient clinic for between February 2023 to December 2025. NGS sequencing was performed using Custom “Fever & Autoinflammatory Disease” panel (SOPHIA Genetics) on an Illumina MiSeq platform. The panel covers the coding regions of 17 genes ( ADA2, CARD14, ELANE, IL10RB, IL10RB, IL1RN, LPIN2, MEFV, MKV, NLRP12, NLRP3, NLRP7, NOD2, PSMB8, PSTPIP1, TNFRSF11A, TNFRSF1A ). Variant calling and data analysis were performed by the Sophia-DDM-V6.5 pipeline. Variant interpretation followed the 2015 ACMG standards and guidelines.
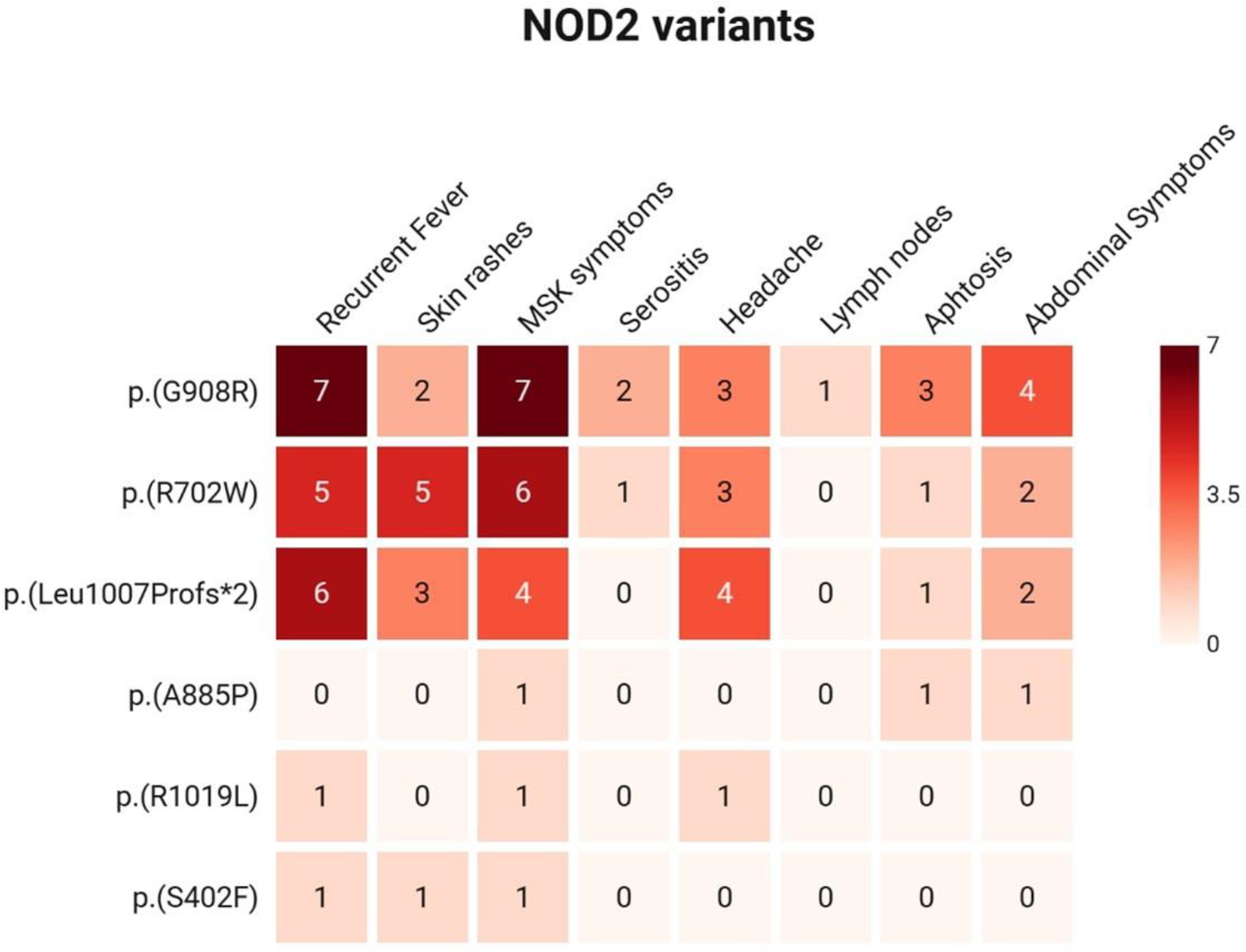
Results: A total of 135 patients (80 females; mean age 37.08 ± 14 years) were enrolled. Of these, 115 patients (85.1%) carried at least one retained non-synonymous variant with a minor allele frequency (MAF) ≤ 0.05. Among them, 25 patients (18%) harbored at least one NOD2 variant classified as pathogenic or as a variant of uncertain significance (VUS). The identified NOD2 variants included heterozygous p.G908R (8 patients), p.R702W (7 patients), p.Leu1007Profs*2 (7 patients), p.A885P (1 patient), p.R1019L (1 patient), and p.S402F (1 patient). The clinical features associated with each variant are detailed in Figure 1 .
Eight of the 25 patients (32%) presented with recurrent fever and skin rashes, along with at least one additional symptom (such as abdominal pain, serositis, arthritis/arthralgia, or sicca manifestation), which may be compatible with a Yao syndrome–like clinical phenotype [1]. The remaining patients did not fully meet the established diagnostic criteria. Two main clinically defined patient groups were identified: one characterised by the p.G908R variant and the other by the p.R702W variant. Almost all patients in both clusters experienced recurrent fever and musculoskeletal symptoms, including arthritis, arthralgia, and myalgia. Abdominal pain was observed in 50% of patients carrying the p.G908R variant, whereas skin rashes were more prevalent among those with the p.R702W variant (71%). Additionally, 57% of patients with the p.Leu1007Profs*2 variant reported headache. About additional genetic findings, among the p.G908R carriers, 5 out of 8 patients also harbored VUS in MEFV gene (3 patients), one had a pathogenic variant in ADA2 , and one had a variant in LPIN2 . Among p.R702W carriers, one patient presented a heterozygous MEFV variant. For those with the p.Leu1007Profs*2 variant, one patient had a co-variation in NOD2 (p.R439C) and another had a pathogenic variation in ADA2 . Additionally, one patient with the p.A885P variant also harbored a VUS in ELANE . The two patients with pathogenic variations in ADA2 did not exhibit typical features of DADA2 and responded adequately to colchicine. All patients with additional VUS in MEFV showed a favourable response to colchicine. Granulomatous skin lesions developed in only one patient with the p.S402F variant, while ascertained inflammatory bowel disease was observed in a patient with the p.Leu1007Profs*2. The coexistence of additional variants in autoinflammatory genes supports a potential oligogenic or modifier-gene contribution to disease expression. Regarding treatment, patients with two VUS across the same or different genes (13 out of 25, or 52%) generally experienced a higher burden of inflammatory symptoms. Eight of these patients had a satisfactory response to colchicine, and in three cases, a combination of colchicine and IL-1 inhibitors resulted in a better clinical outcome.
Conclusions: The use of validated targeted NGS panel is essential for identifying variants that can support or refine clinical diagnosis in autoinflammatory disorders. NOD2-related diseases encompass a wide range of conditions that may not always align with established diagnostic categories such as Yao syndrome, Blau syndrome, or Crohn’s disease. Although patients carrying VUS are typically classified as having uSAID due to uncertain variant pathogenicity, the identification of patient clusters sharing the same NOD2 variants and exhibiting overlapping clinical profiles suggests the existence of previously unrecognized gene-related entities. Further investigations, including whole-exome sequencing and functional studies, are warranted to refine diagnostic frameworks and improved genotype-phenotype interpretation in individuals with NOD2 variants.
Heatmap illustrating the prevalence of the main clinical features associated with each NOD2 variant detected after NGSseq
REFERENCES: [1] Yao Q, Shen M, McDonald C, Lacbawan F, Moran R, Shen B. NOD2- associated autoinflammatory disease: a large cohort study. Rheumatology (Oxford). 2015;54:1904-1912.
Acknowledgments: NIL.
Disclosure of Interests: Marta Schermi: None declared, Maria Teresa Perez-Cartier Beingolea: None declared, Samuele Rizzo: None declared, Anna Fu: None declared, Stefania Moz: None declared, Paola Galozzi: None declared, Roberta Ramonda Novartis, UCB, Takeda, Paolo Sfriso Sobi, Novartis, Sara Bindoli Sobi, Novartis.