fetching data ... 
Background: Rheumatoid arthritis (RA) has been extensively studied to characterize systemic inflammatory signatures and pathways associated with disease onset and treatment response. However, most proteomic studies have focused on RA alone, without direct comparison to other inflammatory arthritides [1-3]. As a result, it remains unclear which molecular features identified in RA reflect RA-specific disease biology and which may represent shared inflammatory signatures across related conditions, such as psoriatic arthritis (PsA). To our knowledge, RA has not been directly compared with PsA using high-dimensional Olink plasma proteomics, particularly in a longitudinal treatment-response setting. Defining shared and distinct underlying pathogenetic programs between RA and PsA could reveal common mechanisms driving inflammatory arthritis, as well as processes associated with disease activity, potentially leading to more effective treatment strategies.
Objectives: To determine whether high-dimensional targeted plasma proteomics can define disease-specific and shared protein signatures in active RA compared with PsA as a disease control and to identify longitudinal proteomic changes associated with disease activity following treatment.
Methods: Plasma samples from 20 patients with active RA, 15 patients with active PsA and 13 sex- and age-matched healthy controls, were analyzed at baseline. Longitudinal plasma samples were collected from 21 patients (11 RA and 10 PsA) after three months of treatment, including patients in whom disease became clinically inactive (n=11; 5 RA and 6 PsA) and those in whom remained active (n=10, 6 RA and 4 PsA). Proteomic profiling was performed using the Olink Explore 384 Inflammation panel. Differential protein expression was assessed using limma and pathway enrichment was performed using gene set enrichment analysis (GSEA) with Gene Ontology and KEGG.
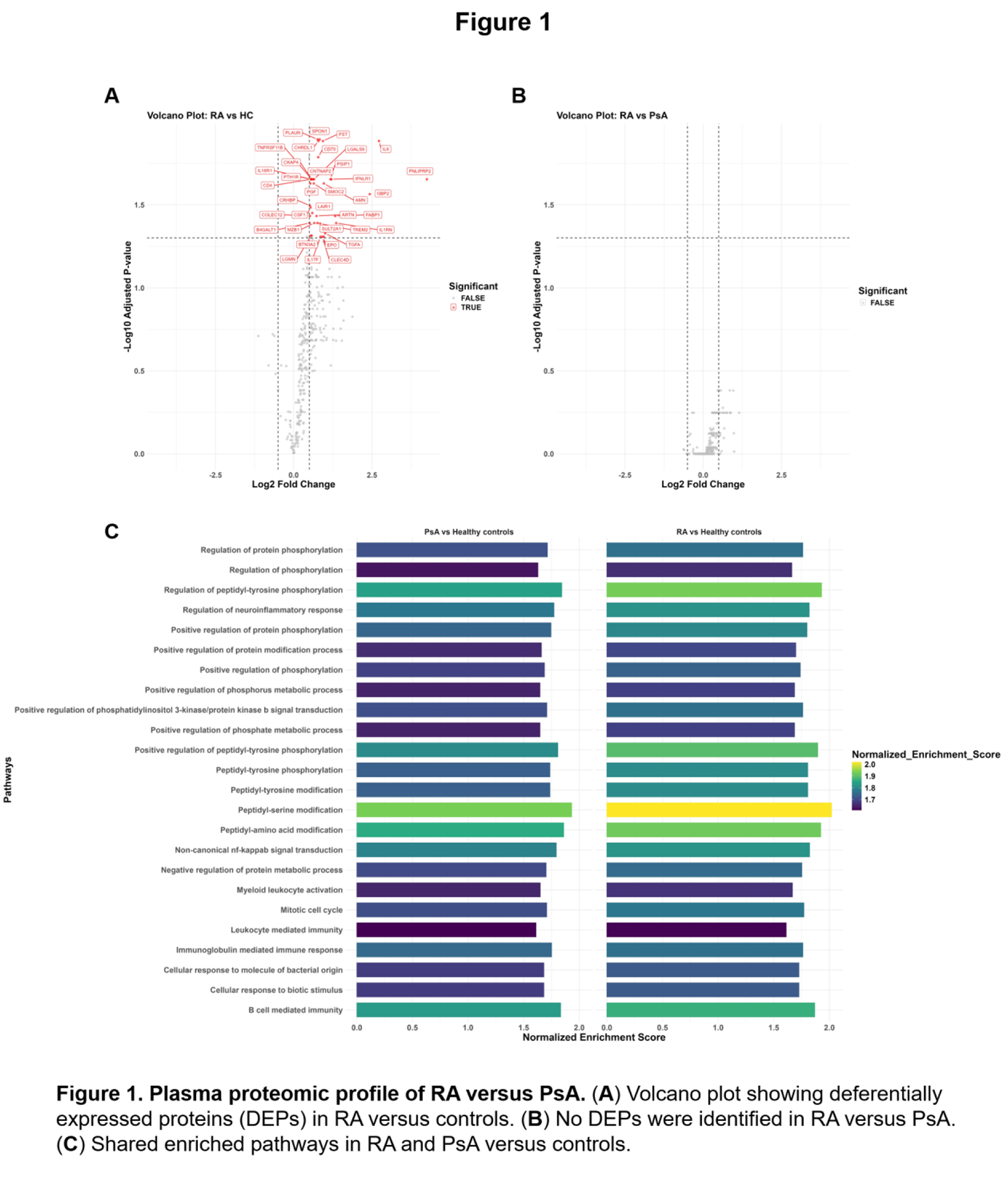
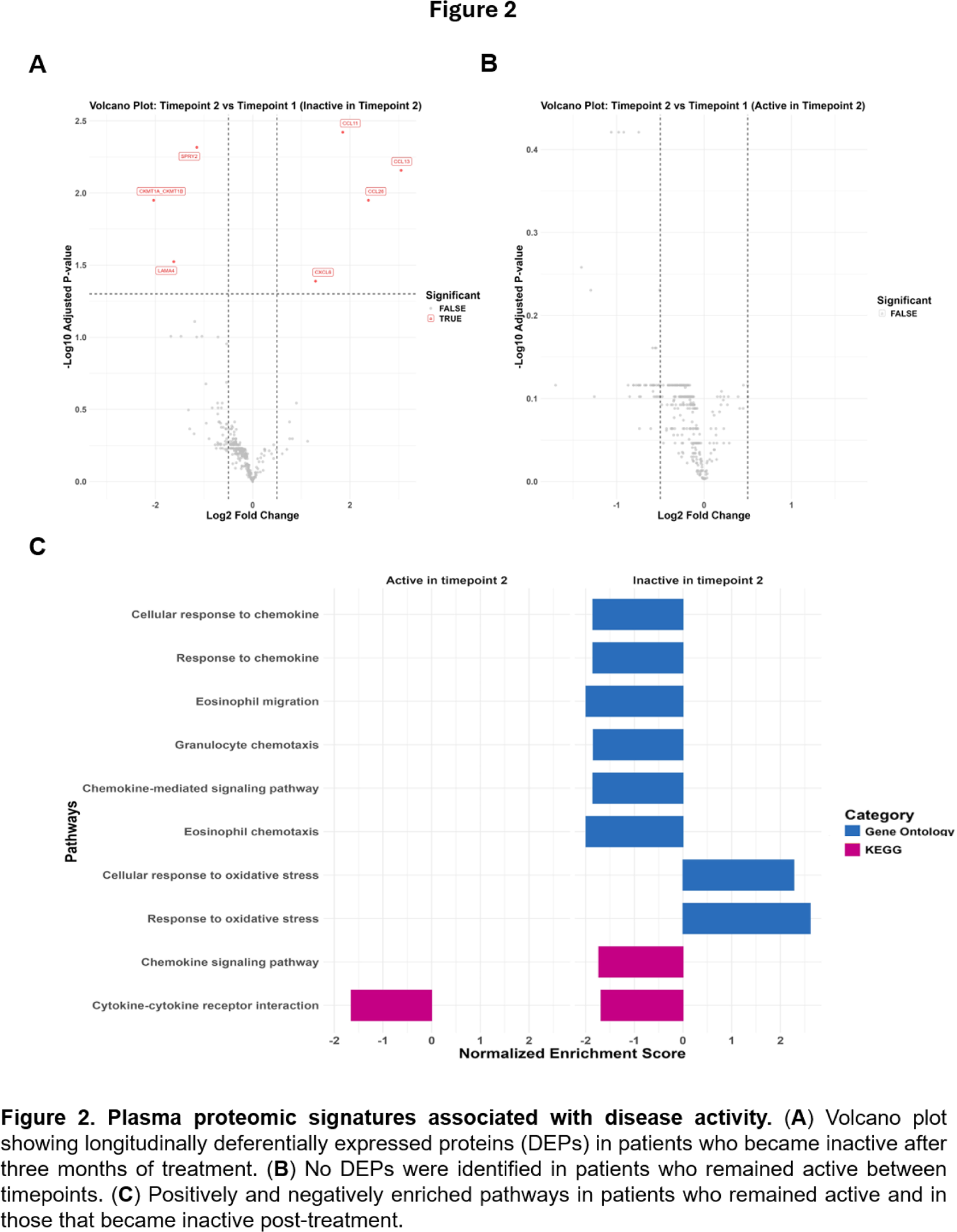
Results: In line with published results [1], differential protein expression analysis at baseline revealed 39 differentially expressed proteins (DEPs) in plasma from patients with RA compared with healthy controls, reflecting increased immune signaling, myeloid and lymphocyte activation, as well as tissue remodeling processes and cell migration (Figure 1A). Notably, no DEPs were identified between RA and PsA (Figure 1B). Pathway analysis demonstrated that RA and PsA shared a substantial overlap in inflammatory pathways, dominated by protein phosphorylation and kinase-driven signaling, immune activation and non-canonical NF-κB-associated processes (Figure 1C). In parallel, disease-specific pathway enrichments were observed, with RA emphasizing cellular remodeling and degradation of structural components and PsA showing distinct chemokine production and regulation, indicating disease-specific programs layered on top of a shared signaling backbone. Given the high degree of proteomic overlap between RA and PsA, patients from both groups were analyzed together in the subsequent longitudinal analysis post-treatment. After three months of antirheumatic treatment according to standard guidelines, differential protein expression was observed exclusively in patients who achieved low disease activity (inactive). Seven plasma proteins were differentially expressed in inactive patients (Figure 2A), including upregulation of certain chemokines (CCL11, CCL13, CXCL6, CCL26) and downregulation of proteins involved in intracellular signaling feedback, endothelial interactions and metabolic activity (SPRY2, LAMA4, CKMT1A/CKMT1B, respectively). No significant proteomic changes were detected in patients who remained clinically active (Figure 2B). Pathway enrichment analysis revealed that suppression of cytokine-cytokine receptor interaction was observed regardless of disease activity, indicating a general treatment effect (Figure 2C). In contrast, only inactive patients showed downregulation of chemokine response and immune cell trafficking pathways, alongside upregulation of oxidative stress response pathways, consistent with immune reprogramming and cellular adaptation. Notably, kinase- and phosphorylation-related pathways identified at baseline were not significantly altered following treatment.
Conclusions: Plasma proteomics revealed that patients with active RA display a distinct inflammatory signature compared with healthy controls, while exhibiting substantial systemic overlap with patients with active PsA. Both diseases share a common kinase-driven inflammatory backbone, likely reflecting disease-intrinsic signaling programs, critical for leukocyte and fibroblast activation and migration. Clinical inactivity was associated with increased metabolic remodeling and reduced chemokine-mediated immune cell trafficking, rather than reversal of core kinase signaling pathways. Further studies may provide additional insights into pathogenic processes underlying inflammatory arthritis, highlighting opportunities to refine therapeutic strategies for both RA and PsA.
REFERENCES: [1] Álvez MB, Bergström S, Kenrick J, et al. A human pan-disease blood atlas of the circulating proteome. Science. 2025;390(6779):eadx2678. doi:10.1126/science.adx2678.
[2] Rachid Zaim S, Savage AK, Gillespie MA, et al. Serum Proteomic Signatures Before the Diagnosis of Rheumatoid Arthritis: Evolving Biologic Pathways and Specific Periods of Disease Development. Arthritis Rheumatol. 2025;77(9):1166-1178. doi:10.1002/art.43175.
[3] Cuesta-López L, Escudero-Contreras A, Hanaee Y, et al. Exploring candidate biomarkers for rheumatoid arthritis through cardiovascular and cardiometabolic serum proteome profiling. Front Immunol. 2024;15:1333995. Published 2024 Feb 14. doi:10.3389/fimmu.2024.1333995.
Acknowledgments: NIL.
Disclosure of Interests: None declared.