fetching data ... 
Background: Immunoglobulin G4-related disease (IgG4-RD) is a systemic fibroinflammatory condition that typically responds well to glucocorticoid treatment. However, relapses occur in up to half of patients during glucocorticoid tapering, leading to cumulative organ damage, prolonged glucocorticoid exposure, and an increased burden of treatment-related adverse effects. Despite several proposed clinical and serological predictors, robust biomarkers that reliably identify relapse-prone patients before induction therapy remain lacking. Given the central role of dysregulated T-B cell interactions in IgG4-RD, detailed immune profiling should hold the key to uncovering relapse-driving immune signatures.
Objectives: We aimed to identify reliable and pathological immune biomarkers capable of predicting future relapse in patients with IgG4-RD.
Methods: We prospectively enrolled consecutive 74 patients with active IgG4-RD who fulfilled the 2011 comprehensive diagnostic criteria, and/or the 2020 revised comprehensive diagnostic criteria, and/or the 2019 American College of Rheumatology/European League Against Rheumatism classification criteria. Age- and sex-matched 22 healthy donors were included as controls. Using multicolor flow cytometry, we conducted comprehensive immunophenotyping of fresh whole blood samples before initiating remission induction therapy. Immunophenotyping included 64 immune cell subsets (T cells subsets, B cell subsets, monocyte subsets, NK cell subsets, neutrophil subsets, eosinophil subsets, basophil subsets, and dendritic cell subsets). Specifically, T peripheral helper (Tph) cells were defined as CD3 + CD4 + CXCR5 - CD45RA - PD-1 high cells. Tph cell subsets were further divided into Tph1 cells (CXCR3 + CCR6 - ), Tph2 cells (CXCR3 - CCR6 - CCR4 + ), Tph17 cells (CXCR3 - CCR6 + ) or Tph1-17 cells (CXCR3 + CCR6 + ) [1]. Furthermore, tissue samples obtained from involved organs were evaluated for detecting immune cell subsets by immunohistochemistry. Relapse of the disease was defined as deterioration of involved organs or emergence of new organ involvements detected by physical, laboratory, and/or imaging tests that required increase of glucocorticoids and/or additional immunosuppressive therapy. An isolated elevation of serum IgG4 levels in the absence of corresponding clinical and/or radiological findings was not considered a relapse. Patients were stratified into relapse and non-relapse groups for comparison.
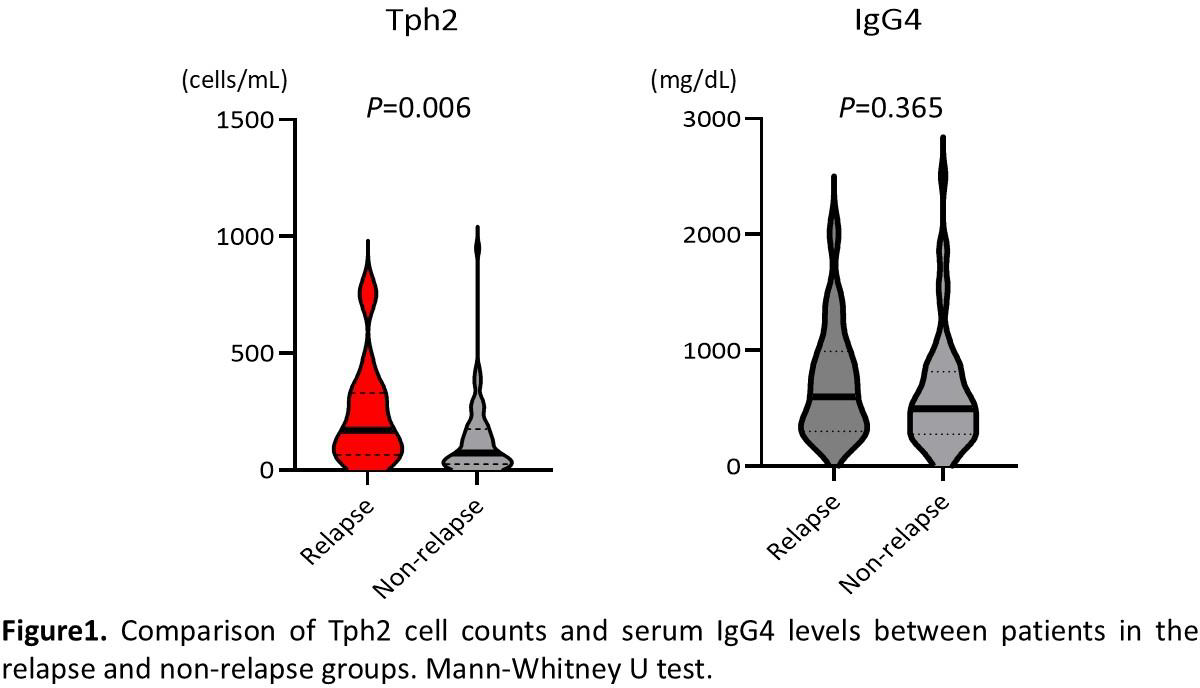
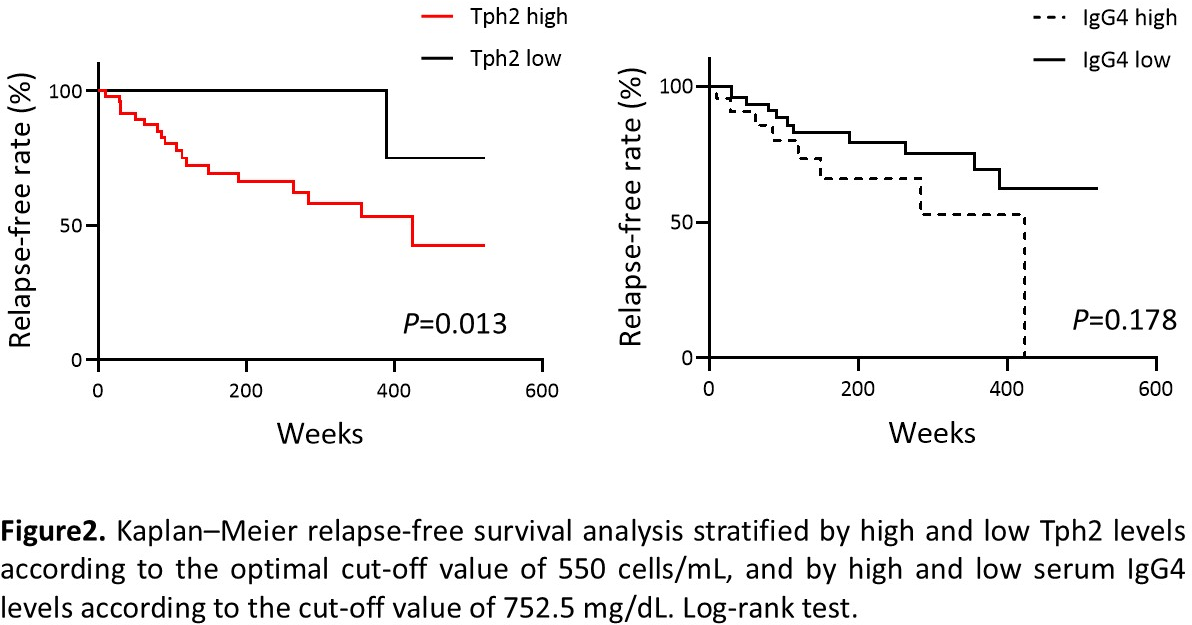
Results: Among 74 patients, 19 (25.7%) experienced relapses, with a median follow-up of 150 weeks. No differences were observed between the relapse and non-relapse groups in the initial glucocorticoid dose at remission induction, the rate of glucocorticoid tapering, or concomitant use of immunosuppressive agents. Patients in the relapse group were younger (48 vs. 66 years, P = 0.040), had more frequent orbit/lacrimal gland involvement (89.5% vs. 63.6%, P = 0.042), and showed lower levels of serum C-reactive protein (0.04 vs. 0.14 mg/dL, P = 0.0019), white blood cell counts (5300 vs. 6100 cells/μL, P = 0.019), and complement components (C3, 87 vs. 98 mg/dL, P = 0.023; C4, 16 vs. 22 mg/dL, P = 0.018), compared with the non-relapse group at the initiation of remission induction therapy. Immunophenotyping revealed a distinct baseline immune signature in patients in the relapse group, characterised by reduced circulating Tfh17 cells (19.9 vs. 28.0 cells/μL, P = 0.017), naïve B cells (41.8 vs. 97.8 cells/μL, P = 0.004), CD19 + B cells (82 vs. 133 cells/μL, P = 0.002), and CD14 + CD16 + monocytes (12.6 vs. 28.2 cells/μL, P = 0.004), with Tph2 cells standing out as the only immune subset that was increased in the relapse group (1800 vs. 900 cells/mL, P = 0.006) (Figure 1). Multivariable logistic regression models that were adjusted for age, sex, and significantly different factors between the relapse and non-relapse groups in the precedent univariate analysis identified Tph2 cell levels as the only independent predictive factor of relapse ( P = 0.029). ROC curve analysis determined Tph2 of 550 cells/mL as the optimal cut-off value, effectively discriminating relapse-free survival (94.1% vs. 16.1%, P = 0.013) (Figure 2). Tph2 cell levels showed significant positive correlations with disease activity by IgG4-RD responder index scores (Rho = 0.261, P = 0.033) and the number of affected organs (Rho=0.309, P =0.011). Although baseline Tph2 cell levels were also positively correlated with baseline serum IgG4 concentrations (Rho=0.353, P =0.003), serum IgG4 levels could not predict future relapse (Figure 1 and 2). Tph2 cell levels were significantly decreased after 12 weeks of glucocorticoid treatment ( P =0.006), along with clinical improvements. Moreover, in the lacrimal gland tissues from patients who experienced relapse, Tph2 cells markedly infiltrated in the extrafollicular regions, compared with those from patients without relapse.
Conclusions: Our comprehensive immune profiling revealed Tph2 cells as a unique relapse-associated immune population in IgG4-RD. Tph2 cells were the only immune subset elevated before remission induction therapy in patients who later relapsed and remained the sole independent predictor of relapse after adjusting for clinical covariates. High Tph2 cell levels strongly correlated with disease burden and IgG4 production, and were accompanied by enhanced extrafollicular infiltration in the affected tissues, highlighting their pathogenic potential. These findings identify Tph2 cells as a promising blood-based biomarker that enables early stratification of relapse-prone patients and provides new insights into the immunopathogenesis of IgG4-RD.
REFERENCES: [1] Seki N, Tsujimoto H, Tanemura S, Kojima S, Miyoshi F, Kikuchi J, et al. Cytotoxic Tph subset with low B-cell helper functions and its involvement in systemic lupus erythematosus. Commun Biol. 2024;7:277.
Acknowledgments: NIL.
Disclosure of Interests: Kanako Shimanuki: None declared, Mitsuhiro Akiyama: None declared, Koichi Saito: None declared, Waleed Alshehri: None declared, Takeru Maruyama: None declared, Takanori Sasaki: None declared, Keiko Yoshimoto: None declared, Noriyasu Seki Tanabe Pharma Corporation, Tanabe Pharma Corporation, Hideto Tsujimoto Tanabe Pharma Corporation, Tanabe Pharma Corporation, kenji Chiba Tanabe Pharma Corporation, Tanabe Pharma Corporation, Yuko Kaneko: None declared.