fetching data ... 
Background: Idiopathic inflammatory myopathies (IIM) and diffuse cutaneous systemic sclerosis (dcSSc) are rare, immune-mediated inflammatory disorders (IMIDs) characterised by substantial morbidity and increased mortality. A substantial proportion of patients remain refractory to available treatments, and durable drug-free remission is rarely achieved. Cluster of differentiation (CD)19-targeted chimeric antigen receptor (CAR)-T cell therapy has shown promise in inducing deep and sustained B cell depletion, potentially enabling an ’immune reset‘ and immunosuppressant-free remission in these IMIDs. This study evaluates rapcabtagene autoleucel (rap-cel; YTB323), a rapidly manufactured autologous CD19-directed CAR-T cell therapy, in patients with severe, refractory IIM and dcSSc.
Objectives: To describe safety and efficacy outcomes in patients with severe, refractory IIM or dcSSc with a follow-up duration up to Week (W) 20 after a single intravenous (i.v.) infusion of rap-cel.
Methods: The Phase 2, open-label, controlled AUTOGRAPH studies in refractory IIM (NCT06665256) and dcSSc (NCT06655896) both include a single-arm safety cohort to assess safety and tolerability of rap-cel (Cohort 1), followed by a randomised cohort (Cohort 2). In Cohort 1 of each study, six eligible IIM or dcSSc patients received protocol-defined lymphodepleting chemotherapy (fludarabine and cyclophosphamide), followed by a single i.v. infusion of rap-cel (12.5 x 10 6 cells). In this preliminary analysis, safety and efficacy outcomes up to W20 post-infusion in patients from Cohort 1 were evaluated.
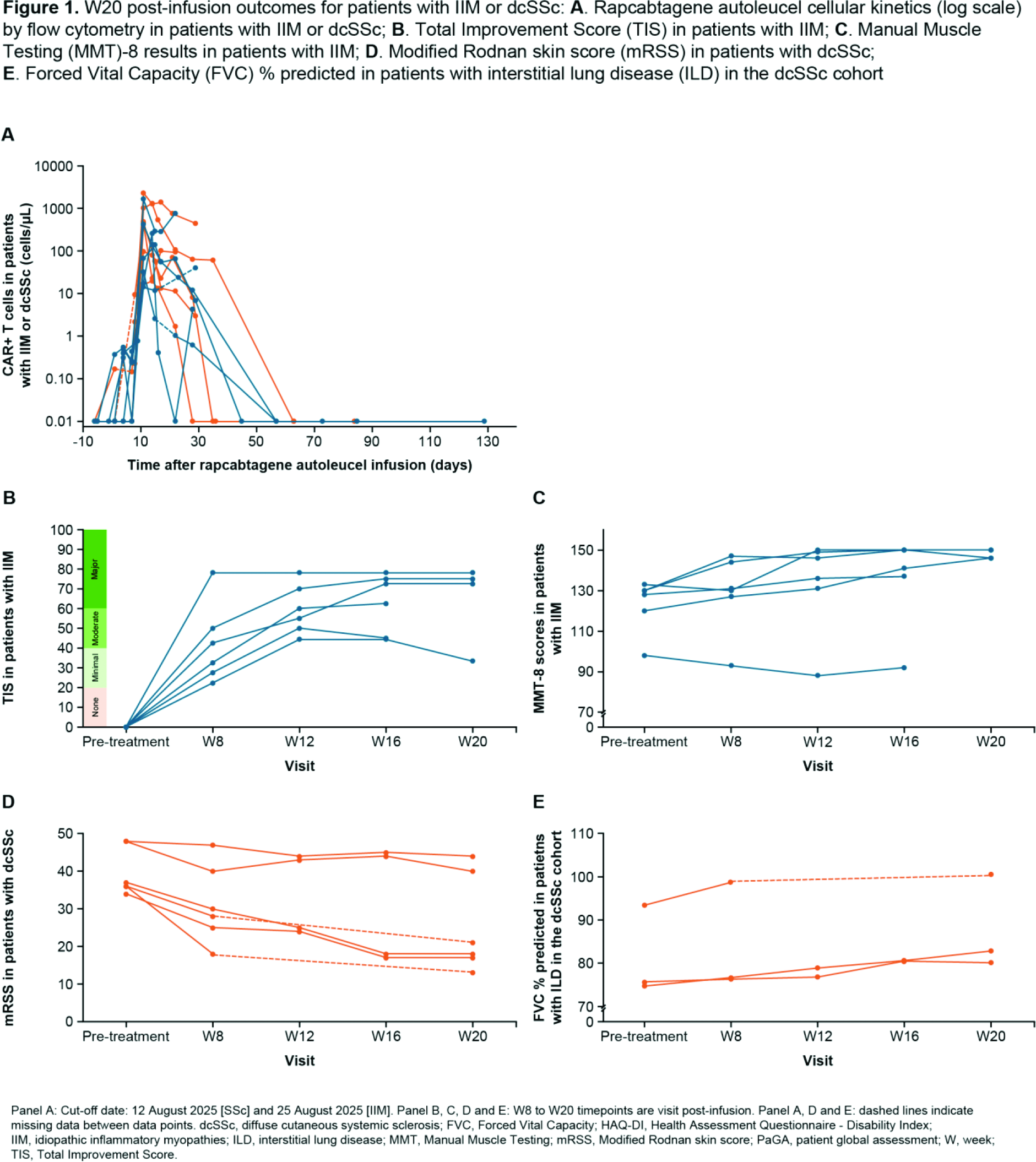
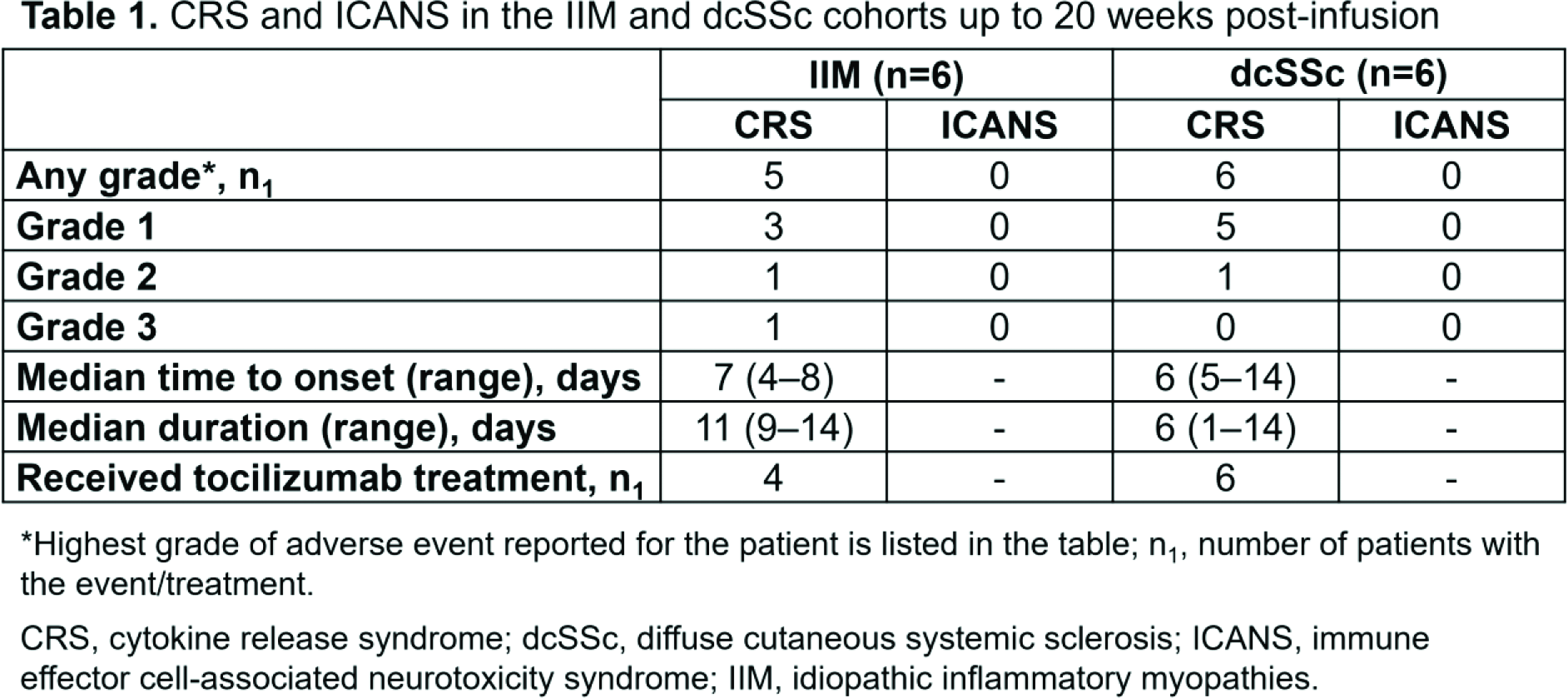
Results: As of the latest data cut-off (IIM: November 2025; dcSSc: December 2025), 4/6 IIM and 6/6 dcSSc patients in Cohort 1 completed the W20 post-infusion assessment; median (range) follow-up post-infusion was 156 (114–270) days for the IIM cohort and 170 (142–311) days for the dcSSc cohort. Cohort 1 of the IIM study included two females; median (range) age was 56 (43–61) years; three patients had anti-synthetase syndrome, two dermatomyositis (DM), and one immune-mediated necrotizing myopathy. All patients had muscle weakness (median manual muscle testing 8 [MMT–8] of 129 [range: 98–133]) and 3/6 had interstitial lung disease (ILD). The dcSSc study included five females; median (range) age was 49 (32–56) years; all had severe skin involvement (median modified Rodnan skin score [mRSS] of 36.5 [range: 34–48]); 3/6 had history of ILD (2/6 meeting progressive ILD criteria) and one had cardiac involvement. Median (range) number of prior therapies was 4.5 (3–9) for IIM and 2.5 (2–4) for dcSSc patients. All patients were positive for IIM- or dcSSc-specific autoantibodies (autoAbs). Median (range) peak CAR-T cell expansion was reached 11 (10–28) days and 10 (10–13) days after infusion in the IIM and dcSSc studies, respectively ( Figure 1A ). Patients demonstrated rapid and complete B cell depletion. B cell reconstitution was observed at 50–100 days post-infusion (n=9/12). Cytokine release syndrome (CRS) occurred in most patients, all Grade (Gr) 1 or 2, except one Gr 3 episode in one IIM patient ( Table 1 ); all resolved without sequelae. Transient (i.e., resolving ≤28 days post-infusion) Gr 3/4 neutropenia was reported in 5/12 patients (two IIM, three dcSSc). Additionally, one case of Gr 4 neutropenia adverse event (AE) with onset at Day (D) 18 post-infusion was reported in a dcSSc patient that resolved to Gr 3 by D33 post-infusion and returned to normal counts by D36. One mild hypogammaglobulinemia event was reported in one dcSSc patient, which did not require any treatment. AEs, including infections, were manageable and aligned with the established safety profile of CAR-T cell therapies. As of the data cut-off, four IIM patients achieved major improvement in Total Improvement Score (TIS), one patient achieved moderate and one minimal improvement in TIS ( Figure 1B ). Median MMT-8 increase from baseline (BL) was 14 points at 12 weeks post-infusion (n=6) and 20 points at 20 weeks post-infusion (n=4; Figure 1C ). At W20 post-infusion, amongst patients with available data, median % relative decrease from BL in Physician Global Assessment (PhGA), Patient Global Assessment (PaGA), and Health Assessment Questionnaire – Disability Index (HAQ-DI) was 76.7 (n=4), 58.4 (n=2) and 16.7 (n=3) respectively. In the two patients with DM, Cutaneous Dermatomyositis Disease Area and Severity Index – Activity (CDASI-A) improved up to the last follow-up (from BL score of 38 to 15 by D56 in one patient, and from 18 to 14 by D141 in the second patient). In the dcSSc cohort at W20 post-infusion, median (range) mRSS score was 19.5 (13–44) and the % relative reduction from BL was 46 (n=6; Figure 1D ); among patients with history of ILD, median % relative improvement from BL in forced vital capacity % predicted was 8 (n=3) and 9 (n=2) for those with progressive ILD ( Figure 1E ); median % relative decrease from BL in PhGA, PaGA and HAQ-DI was 46 (n=6), 52 (n=6), and 47 (n=6), respectively. Composite Response Index in Systemic Sclerosis (rCRISS) 25 and 50 (2/5 components) and 25 and 50 (3/5 components) was achieved in 5/6 and 4/6 patients, and 4/6 and 3/6 patients, respectively, by W20 post-infusion. Marked decreases from BL in dcSSc-specific autoAbs over time were observed in all patients. All patients with IIM or dcSSc discontinued and remained off all immunosuppressants after treatment with rap-cel.
Conclusions: Preliminary data from these safety cohorts show a favourable safety profile, CAR T-cell expansion, complete B cell depletion and promising initial efficacy (improvement in TIS [IIM], mRSS [dcSSc], and lung function [dcSSc]), in patients with severe, refractory IIM or dcSSc, supporting its continued evaluation
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Dinesh Khanna Amgen, Abbvie, AstraZeneca, BMS, Boehringer, Novartis, Xavier Andrade-Gonzalez: None declared, Mark Vercel: None declared, Merav Lidar: None declared, Avichai Shimoni: None declared, Alexander Pfeil: None declared, Ulf Schnetzke: None declared, Gianluca Moroncini: None declared, Francesco Saraceni: None declared, Yves Allenbach: None declared, Sylvain Choquet Novartis, Novartis, Andrea Low Novartis, Boehringer-Ingelheim, Johnson & Johnson, Boehringer-Ingelheim, Johnson & Johnson, Boehringer-Ingelheim, Yunxin Chen Abbvie, Bristol Meyers Squibb, GlaxoSmithKline, Johnson & Johnson, Kite Gilead, Novartis, Takeda, GlaxoSmithKline, Johnson & Johnson, Kite Gilead, Pfizer, Takashi Matsushita: None declared, Akiyo Yoshida: None declared, Marie-Elise Truchetet BMS, Novartis, Celltrion, Lilly, Johnson & Johnson, UCB, AstraZeneca, Novartis, Abbvie, Edouard Forcade Novartis, Alexion, Sobi, Gilead, Sanofi, Jazz, Novartis, Alexion, Ran Nakashima: None declared, Yasuyuki Arai: None declared, John Moore: None declared, Laila Girgis Pfizer, Lidia Sanchez Riera Pfizer, Pfizer, Novartis, Angeliki Giannelou Novartis Pharmaceuticals, Novartis Pharmaceuticals, Yuejia Xu Novartis, Alexandra Kuznetsova Novartis, Fernando Kawakami Novartis, Novartis, Bibha Das Novartis, Chih-Yung Sean Lee Novartis, Ewa Gatlik Novartis, Novartis, Muhsen Alani Novartis, Novartis, Vineeth Varanasi Novartis Pharma AG, Novartis, Susanne Diehl Novartis, Anubhav Mathur Novartis Pharmaceuticals, Novartis Pharmaceuticals, Rohit Aggarwal Abcuro, Alexion, ANI Pharmaceutical, Argenx, Artiva Biotherapeutics, AstraZeneca, Boehringer Ingelheim, Bristol Myers-Squibb, Cabaletta Bio, Capstanx, Century Therapeutics, CSL Behring, Dren Bio, EMD Serono, Fate Therapeutics Inc, Galapagos, GlaxoSmithKline LLC (GSK), Horizontal Therapeutics, Immunovant, Janssen, Janux Therapeutics, Kiniksa Pharmaceuticals, Lilly, Meiji Pharma, Novartis, Nkarta, Octapharma, OneFour Bio, Orna Therapeutics Inc, Ouro Medicines, Pfizer, PRoivant, SOBI, and Sun Pharmaceutical Industries, Boehringer Ingelheim (BI), Cabaletta Bio, Janssen, and PRoivant.