fetching data ... 
Background: Patients with rheumatoid arthritis (RA) are at a lower risk of developing breast and colorectal cancer compared to the general population, whereas evidence of the association between RA and prostate cancer remains inconclusive [1-2]. Genetic mechanisms have been proposed to underlie these associations [2-3]. The impact of RA on the risk of common cancers in individuals with varying genetic susceptibility for these cancers is unknown.
Objectives: To estimate the association between polygenic risk scores for breast, prostate, and colorectal cancer and the risk of the corresponding cancers among patients with rheumatoid arthritis and matched controls.
Methods: Within the FinnGen study containing 519,972 Finnish biobank samples combined with longitudinal nationwide health registry data, we identified patients diagnosed with RA at ages 40-80 between 2000 and 2021 (≥ 2 ICD-10 codes compatible with RA in a hospital discharge registry) and matched them by sex and birth year with up to 20 controls without an inflammatory joint disease. Individuals with breast, prostate, or colorectal cancer before the index date were excluded. Analyses of breast and prostate cancer were restricted to female and male participants, respectively. Follow-up started from RA index date for cases and at an identical age for controls, and ended at diagnosis of the cancer of interest, death, emigration, completion of 15 years, or end of follow-up on December 31, 2022, whichever came first. Kaplan-Meier curves were used to estimate cumulative incidences of common cancers. Hazard ratios (HRs) with 95% confidence intervals (CIs) were estimated by Cox proportional hazards models, adjusted for birth year, the first four principal components of ancestry, and sex (for colorectal cancer analyses). As a sensitivity analysis, we applied Fine–Gray subdistribution hazard models to account for death as a competing risk. Published genome-wide PRSs generated with PRS-CS were used, categorised into 0-20%, 20-80%, and 80-100%.
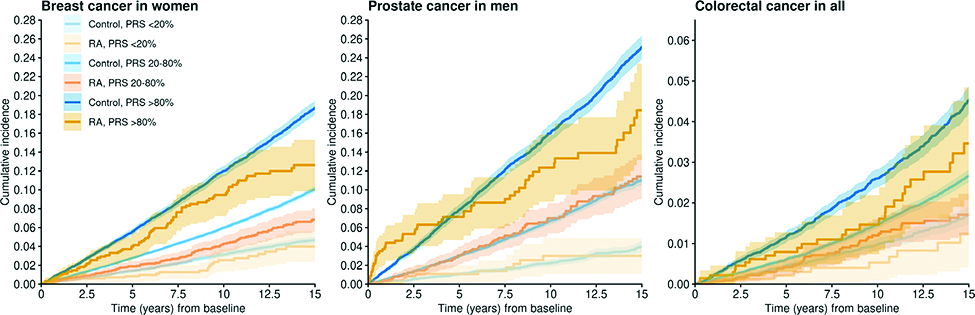
Results: We identified 7,275 RA patients (4810 (66.1%) women, mean (SD) age 59.5 (9.8) years), and 132,870 birth-year and sex-matched controls. PRSs for breast, prostate, and colorectal cancer were similarly associated with the respective cancers in both RA cases and controls. At 15 years, RA was associated with decreased risks of breast cancer (HR 0.70, 95% CI 0.61-0.80) and colorectal cancer (HR 0.69, 95% CI 0.56-0.86) but not prostate cancer (HR 0.90, 95% CI 0.77-1.06). These results were consistent in magnitude and direction in sensitivity analyses using Fine–Gray models accounting for death as a competing risk. The cumulative incidences of the cancers across cancer-specific PRS categories and according to RA status are shown in Figure 1. For the associations of RA and breast and colorectal cancer, the effect sizes remained similar across PRS categories. For breast cancer, HRs (95% CIs) were 0.72 (0.58-0.91), 0.68 (0.57-0.81), and 0.80 (0.53-1.20) within the high, average, and low PRS categories, respectively. For colorectal cancer, HRs (95% CIs) were 0.71 (0.49-1.05), 0.69 (0.52-0.93), and 0.67 (0.36-1.26) within the high, average, and low PRS categories. Among those with high prostate cancer PRS, RA cases had a higher cumulative incidence of prostate cancer compared to non-RA controls during the first few years after RA diagnosis (Figure 1). This risk difference was attenuated and reversed after a longer follow-up (HR 0.77, 95% CI 0.58-1.00). The presence of RA did not alter prostate cancer risk among those with low or average prostate cancer PRS (HRs (95% CIs) were 0.95 (0.50-1.79) and 1.01 (0.82-1.24), respectively). No statistically significant interactions between RA and cancer-specific PRSs were observed with respect to cancer risk at 15 years.
Conclusions: Across the levels of polygenic risk for breast and colorectal cancers, RA patients had a lower risk of the respective cancers. RA patients with a high PRS for prostate cancer may be diagnosed with prostate cancer at a higher rate compared to non-RA controls during the first few years after RA diagnosis, which may be due to a true increase in incidence or surveillance bias. Next, we aim to investigate the underlying mechanisms of these associations, such as environmental, hormonal, pharmacological, and additional genetic factors.
Cumulative incidences and 95% confidence intervals of common cancers across cancer-specific PRS categories among RA cases and non-RA controls.
REFERENCES: [1] Simon TA, Thompson A, Gandhi KK, Hochberg MC, Suissa S. Incidence of malignancy in adult patients with rheumatoid arthritis: a meta-analysis. Arthritis Res Ther. 2015;17:212.
[2] Ou J, Zou L, Wu Y, Zhang Q, Fang Y, Qiu M, Tian X, Ma L, Bi H, Liu C. Causal inference between rheumatoid arthritis and prostate cancer. Clin Exp Med. 2023;23:4681-4694.
[3] Wadström H, Pettersson A, Smedby KE, Askling J. Risk of breast cancer before and after rheumatoid arthritis, and the impact of hormonal factors. Ann Rheum Dis. 2020;79:581-586.
Acknowledgments: NIL.
Disclosure of Interests: Virva Kuusi: None declared, Anne Kerola has received speaker’s honoraria from Abbvie, Boehringer-Ingelheim, and Novartis, Eirik Ikdahl has received speaker’s honoraria from Boehringer Ingelheim, Finngen FinnGen: None declared, Nina Mars: None declared.