fetching data ... 
Background: Systemic sclerosis (SSc) is an autoimmune disease characterized by inflammation, vascular injury and excessive fibrosis in different organs. Semaphorin 4A (Sema4A) is a transmembrane protein that belongs to a large family of proteins initially described as ligands essential for neuronal development. Previous studies from our group have shown that Sema4A is elevated in patients with SSc and it promotes in vitro CD4 + T cell-mediated inflammation and fibrosis.
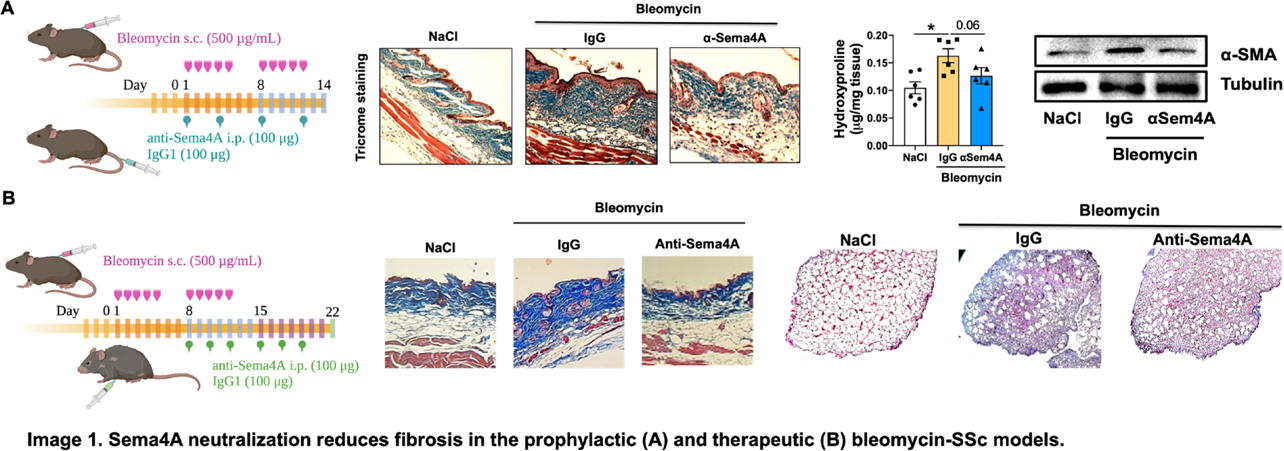
Objectives: The aim of this study is to determine the effect of Sema4A neutralization in a 3D model of immunity-driven fibrosis and in the bleomycin-induced SSc mouse model.
Methods: Sema4A plasma levels were measured by ELISA. We used the bleomycin-induced SSc model, in which mice were treated prophylactically (before the onset of fibrosis) or therapeutically (after the onset of fibrosis) with an anti-Sema4A neutralizing antibody or its respective IgG isotype control. The 3D cell culture model, consisting in a collagen hydrogel, dermal fibroblast from healthy controls (HC), and HC or SSc peripheral blood mononuclear cells (PBMCs), was stimulated with SSc serum in the presence of an anti-human Sema4A antibody or its respective IgG isotype control. Collagen content was determined by Mason’s trichrome staining and hydroxyproline assay. Protein and mRNA expression was determined by RT-qPCR, immunohistochemistry and immunoblotting. Cytokine production by CD4 + and CD8 + T cells from draining lymph nodes was determined by flow cytometry.
Results: The prophylactic and the therapeutic administration of the anti-Sema4A antibody significantly reduced skin and lung collagen content in the bleomycin-SSc mice, compared to the IgG control group. This effect accompanied by diminished mRNA and protein expression of extracellular matrix (ECM) components and fibrotic mediators, most notably smooth muscle actin (α-SMA). Anti-Sema4A treatment also attenuated the mRNA expression of inflammatory mediators and the immune cell infiltration in the affected tissues, as well as the Th2 and Th17 cell cytokine production within draining lymph nodes.
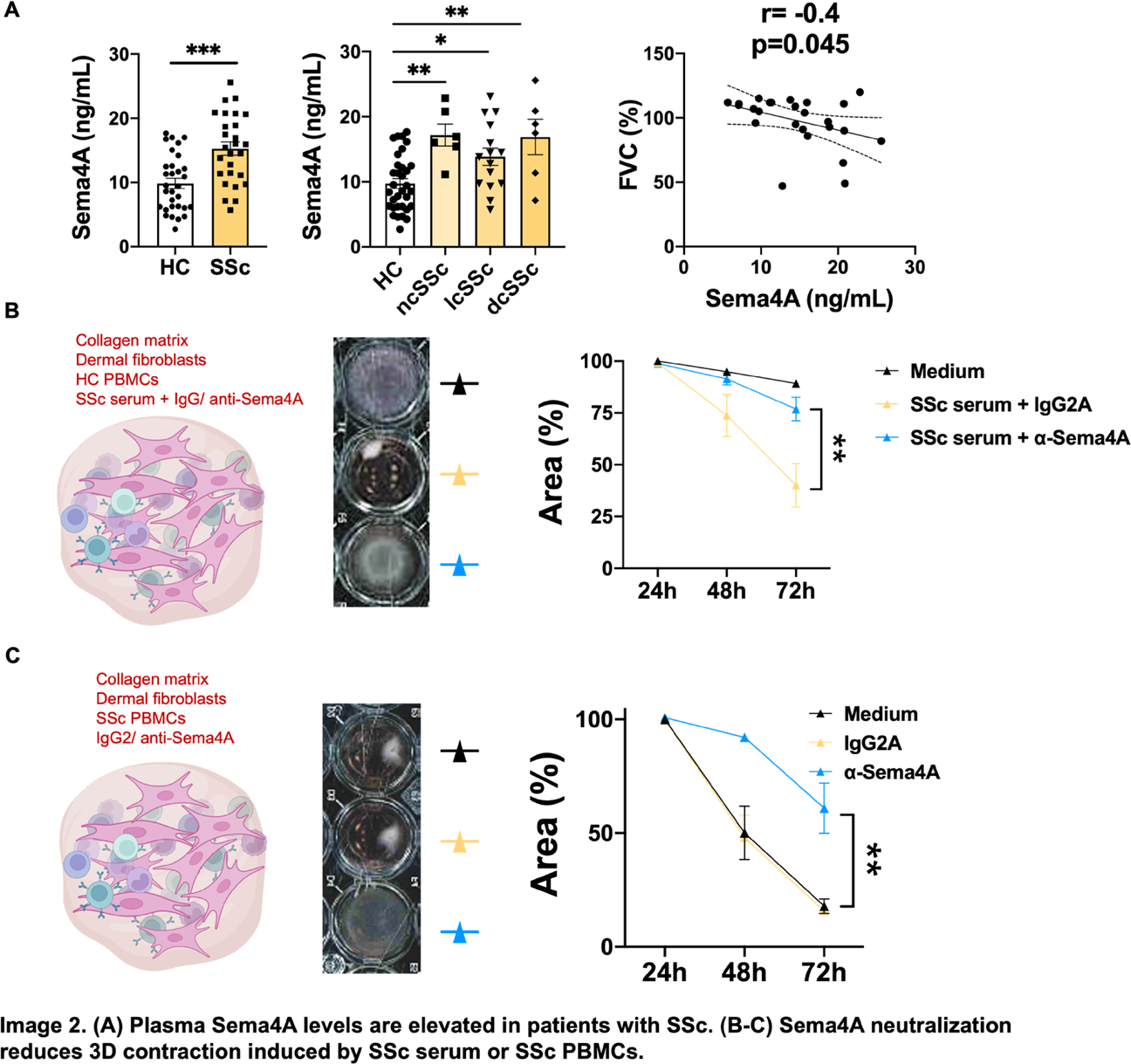
In our cohort of patients, we confirmed the elevated Sema4A levels in patients with SSc, which negatively correlated with the forced vital capacity (FVC). Consistent with the in vivo findings, Sema4A neutralization exerted a comparable anti-fibrotic effect in the 3D culture model. The serum and the PBMCs of patients with SSc induced contraction of the 3D model, which was drastically abrogated by the addition of an anti-human Sema4A antibody. Moreover, a reduced mRNA expression of ECM members and fibrotic mediators was also observed, as well as a reduced α-SMA protein expression.
Conclusions: Our findings confirm the pro-fibrotic and pro-inflammatory role of Sema4A in SSc, postulating Sema4A neutralization as a novel therapeutic approach for the treatment of this devastating disease.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.