fetching data ... 
Background: Systemic lupus erythematosus (SLE) is a chronic autoimmune disease marked by immune dysregulation, which predisposes patients to severe infections. Infections remain a leading cause of morbidity and premature mortality among SLE patients. Although SLE patients are known to have an elevated average risk of severe infection, little is known about how this excess risk varies by personal characteristics of each SLE patient. While these reported average relative risk estimates provide important insights into the overall impact of SLE exposure, relying solely on such average exposure effects can be inadequate because they can mask the possibility that certain subgroups of patients experience a disproportionately higher risk of infection and mortality, while others may be less affected. The clinical impacts of SLE are unlikely to be uniform and can depend on individual characteristics such as age, sex, socioeconomic status, prior infections, comorbidities, and medication exposure. Identifying specific risk modifiers that place certain patients at disproportionately higher risk is essential for personalized risk assessment. However, traditional models often struggle to capture the complex, non-linear interactions between these high-dimensional modifiers, necessitating advanced data-driven approaches.
Objectives: The primary objective of this study was to quantify the individual-level heterogeneity in the excess severe infection rate attributable to SLE within a large, population-based cohort. Specifically, we aimed to: [1] estimate personalized excess infection risk (Conditional Average Exposure Effects) to reveal the distribution masked by population averages; and [2] identify and characterize the key clinical, demographic, and socioeconomic risk modifiers that drive disproportionate vulnerability among SLE patients.
Methods: We conducted a population-based matched cohort study using health administrative data from British Columbia, Canada (1990–2024). We identified incident SLE patients using a validated algorithm and matched them 1:5 to non-SLE controls based on birth year, sex, and index year. To measure the heterogeneity of infection risk, we employed Causal Forests to estimate personalized excess infection risk for each SLE patient. Generalized Additive Models were used to characterize the potentially non-linear relationships between patient profiles and the estimated excess risk of severe infection.
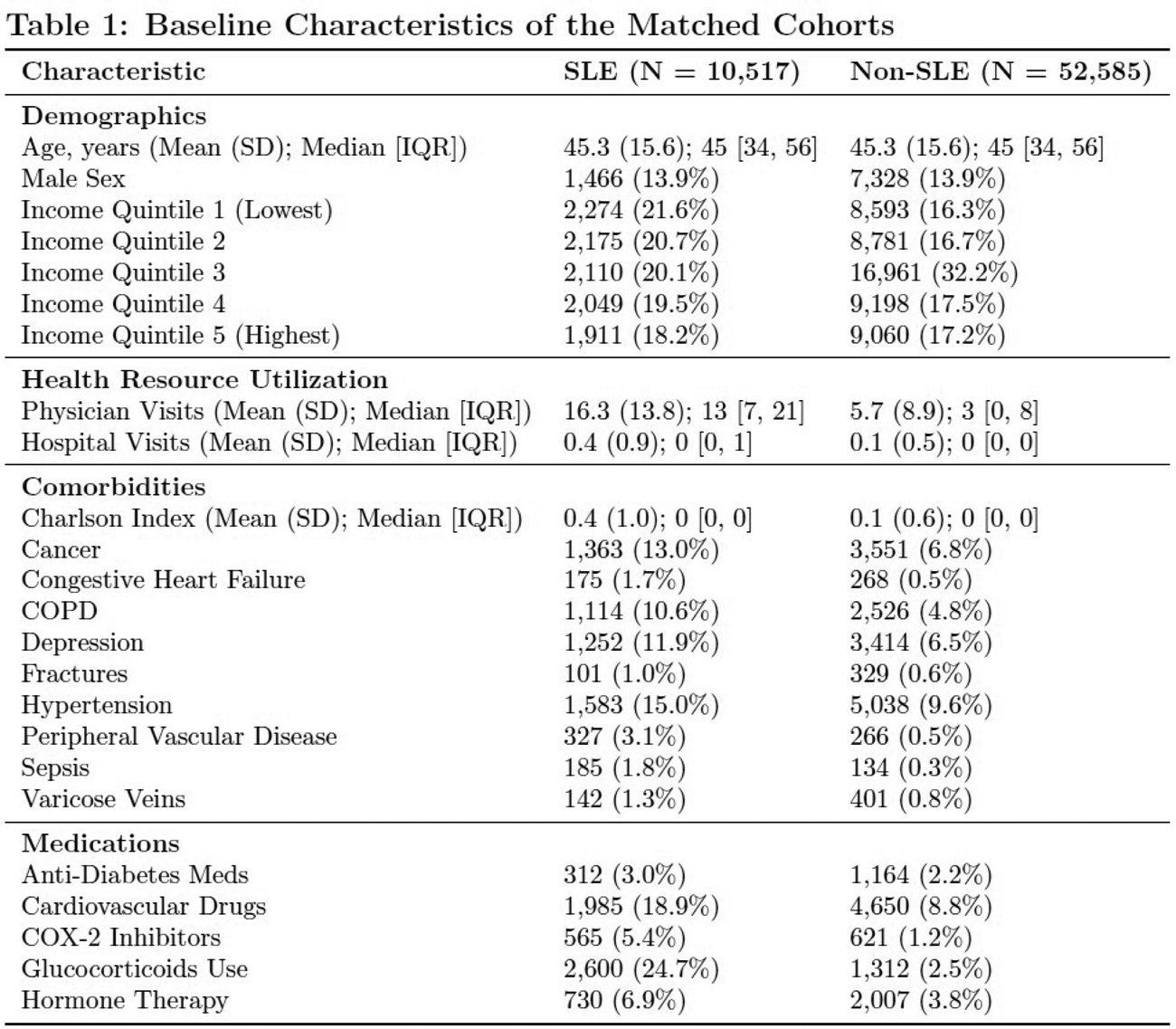
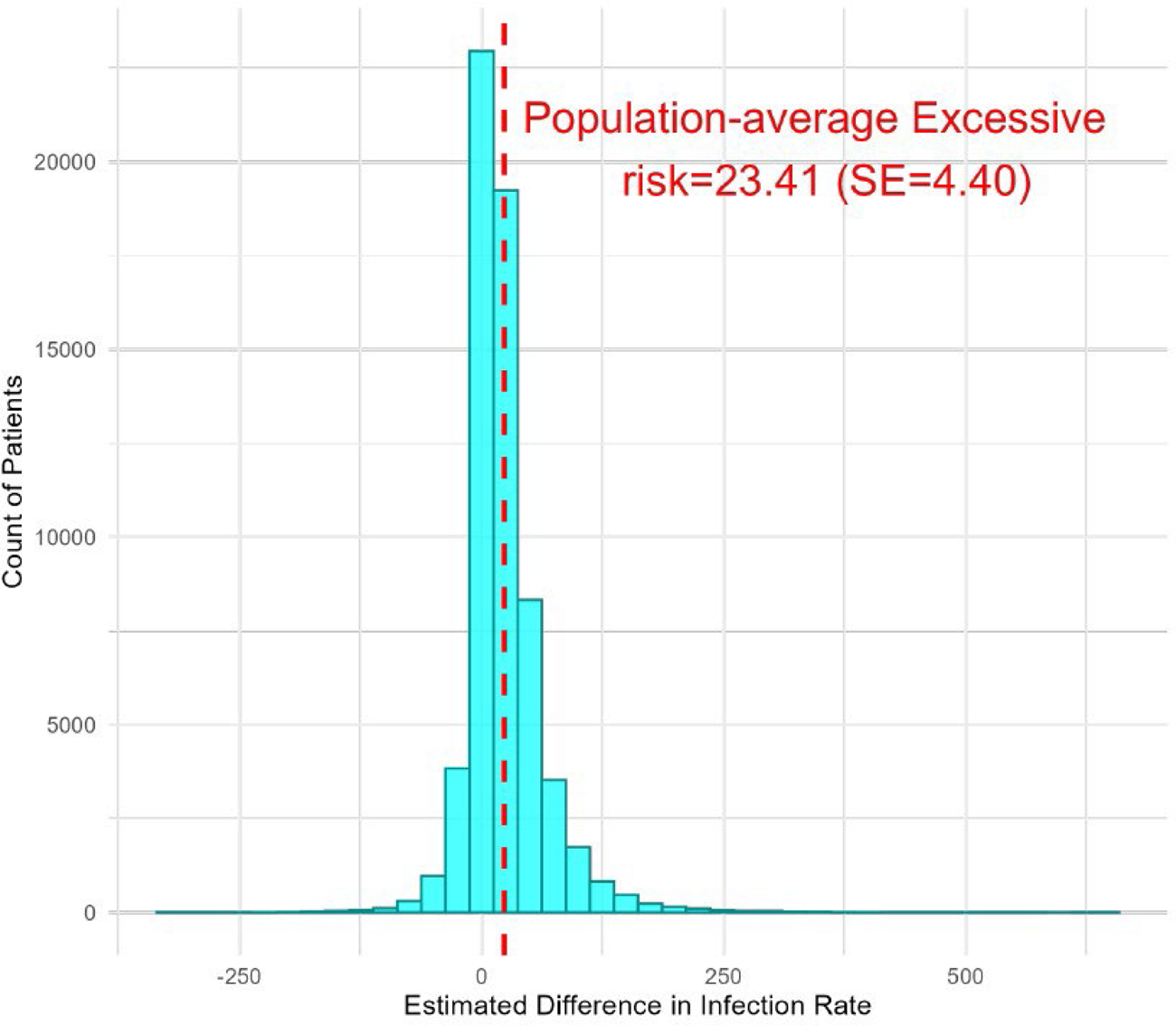
Results: We identified 10,517 incident SLE patients matched to 52,585 non-SLE controls (Table 1). While cohorts were identical in age (mean 45.3 years) and sex (13.9% male), SLE patients exhibited significantly higher baseline healthcare utilization (mean 16.3 vs. 5.7 physician visits) and comorbidity burden (mean CCI 0.4 vs. 0.1). Using causal forests, we estimated a population-average excess severe infection risk of 23.41 (SE: 4.40) per 1,000 person-years among SLE patients. While this average is significant, individual-level estimates revealed substantial heterogeneity, ranging from -329.42 to 639.29 per 1,000 person-years (SD: 40.60) (Figure 1). Variable importance analysis identified baseline physician visits, hospitalizations, and age as the most influential risk modifiers. Specifically, the excess infection rate increased with outpatient utilization, while frequent hospitalization (>15 visits) was associated with a sharp increase in risk. Age followed a U-shaped pattern, with the highest additional risk observed in the youngest and oldest SLE patients. Key worsening factors included depression (+20.21 per 1,000 person-years) and rural residence (+13.79), while higher income and hypertension were associated with an attenuating effect on excess risk of severe infection rate.
Conclusions: Significant disparities exist in excess risk of severe infection rate associated with SLE. Focusing only on population-average risk can obscure vulnerable subgroups with disproportionately high infection rates. Modern causal machine learning methods can support personalized risk stratification, helping clinicians move beyond average risk estimates toward targeted surveillance and prevention for high-risk SLE patients. The impact of SLE on severe infection risk is not uniform, but a wide distribution modified by personal characteristics. By leveraging a data-driven causal forest framework, we demonstrated that the population-average risk masks important vulnerable subgroups of patients with a disproportionately high infection rate. We identified age, healthcare utilization and comorbidities such as depression and heart failure as key modifiers. These findings lay a robust foundation for personalized risk stratification and suggest that clinicians should move beyond average risk assessments and implement personalized surveillance and preventive strategies for such SLE patients with high-risk profiles. This study illustrates the unique power of combining large-scale health administrative data with causal machine learning to translate real-world evidence into a personalized rheumatological treatment regimen.
REFERENCES: [1] M. Petri. Infection in systemic lupus erythematosus. Rheumatic Diseases Clinics of North America, 24(2):423–456, May 1998.
[2] Kai Zhao, Hui Xie, Lingyi Li, John M Esdaile, and J Antonio Aviña-Zubieta. Increased risk of severe infections and mortality in patients with newly diagnosed systemic lupus erythematosus: a population-based study. Rheumatology, 60(11):5300–5309, November 2021.
[3] Bilal Hasan, Alice Fike, and Sarfaraz Hasni. Health disparities in systemic lupus erythematosus-a narrative review. Clinical Rheumatology, 41(11):3299–3311, November 2022.
Acknowledgments: NIL.
Disclosure of Interests: None declared.