fetching data ... 
Background: The evaluation of children with septic arthritis (SA) and or acute hematogenous osteomyelitis (AHO) is challenging due to the high rate of negative cultures and the consideration of other inflammatory and genetic conditions. Current clinical and laboratory parameters do not reliably differentiate acute mono-arthritis cases between infectious, inflammatory, or autoimmune arthritis early on, which necessitates ongoing follow-up and presumptive antibiotic therapy while observing for resolution or evolution toward alternative diagnostic considerations(delayed diagnosis). Existing methods are optimized around adult population, interms of specimen volume requirement and turnaround-time.
Objectives: The goal of present study was to identify immune biomarkers for rapid screening of blood and joint-fluid specimens to guide the clinical decision-making for children suspected to have presumed septic arthritis (SA), acute hematogenous osteomyelitis (AHO) or other underlying autoimmune or genetic conditions. Aim was to identify the early immune correlates of bacterial infection verses autoimmune pathology driven arthritis in children.
Methods: We performed single cell RNA sequencing and IgG antibody repertoire screening in knee joint-fluid specimens of 20 children diagnosed with presumed septic arthritis and or AHO. Standard of care culture and metagenomic sequencing was performed to profile the microbiome. We screened anti-IgG and IgM antibody signatures against a panel of 120 autoantigens previously implicated in several rheumatic and autoimmune conditions. Microbiome data was analyzed using 16S analysis module. Single cell RNA-seq data was analyzed using 10X Genomics cell-ranger and loupe browser pipelines. Cytokine and autoantibody data was analyzed using parametric and non-parametric methods in GraphPad prism software. We also screened microbial and autoantibody signatures in a healthy cohort of 234 young children. A proof-of-concept multi-omics approach that combined metagenomics, single cell transcriptomics, cytokine and autoantibody data was applied to profile the microbes and host immune factors in the knee joint of affected children.
Results: Metagenomic sequencing confirmed the presence of Streptococcus pyogenes and Staphylococcus aureus species in 50% of the joint fluids. The remaining 50% patients were negative for any infectious pathogen. Inflammatory cytokines including IL-4, IL-17A, MCP-1, IL-8, IL-2, IL-1b, IL-6, TNF-a, etc. were significantly (p<0.05) elevated in the children with bacteremia as compared to infection negative subset. Interestingly, children without any bacteremia exhibited strong signatures of autoantibodies (IgGs) targeting several nuclear i.e. dsDNA, histones, Jo-1, scl-70, Ro/SS-A, SmDs, CENP-A and non-nuclear auto-antigens i.e. Collagens, Myosin, Laminin . Furthermore, single cell transcriptomics in autoantibody positive subset confirmed the abundance of autoreactive Tfh (T follicular helper) and antibody producing class switched B cells in this knee joint-fluid. The single cell data clearly showed distinct immune composition of infection negative and infection positive knee joint fluids in children. The single cell network analysis identified a gene cluster featuring elevated expression of Histone 3 (H3), Retinoic acid-inducible gene I (RIG-I), CRIP1 (Cysteine-rich intestinal protein 1) and LY6E (Lymphocyte antigen 6 family member E) genes to be enriched in the patients with highest platelet counts and ESR. Also, this cluster was associated with high titers of anti-collagens, dsDNA, histones, and sm antibodies. These gene marrkes are previously implicated in rheumatoid arthritis (RA), juvenile idiopathic arthritis (JIA) and SLE (systemic lupus erythematosus) (Figure 1). The antibody repertoire in healthy children was targeted against viral pathogens i.e. RSV (Respiratory syncytial virus).We developed a multiomics pipeline for rapid investigation of microbiome and host immune responses in relation to infectious and autoimmune diseases in Children. Here we show that multi-omics approach guided the diagnosis of three culture negative cases as inflammatory arthritis, Juvenile idiopathic arthritis (JIA) and Post-Streptococcal Reactive Arthritis. Overall, this improved the diagnostic confidence for children with suspected septic arthritis and AHO. This study generated an extensive resource of single cell gene expression data on knee joint-fluid to further investigate the pathways and mechanisms involved in driving clinical disease especially in the infection negative patients.
Conclusions: The multiomics approach rapidly stratifies patients with bacterial infection or potential autoimmunine pathology driven septic arthritis in children.
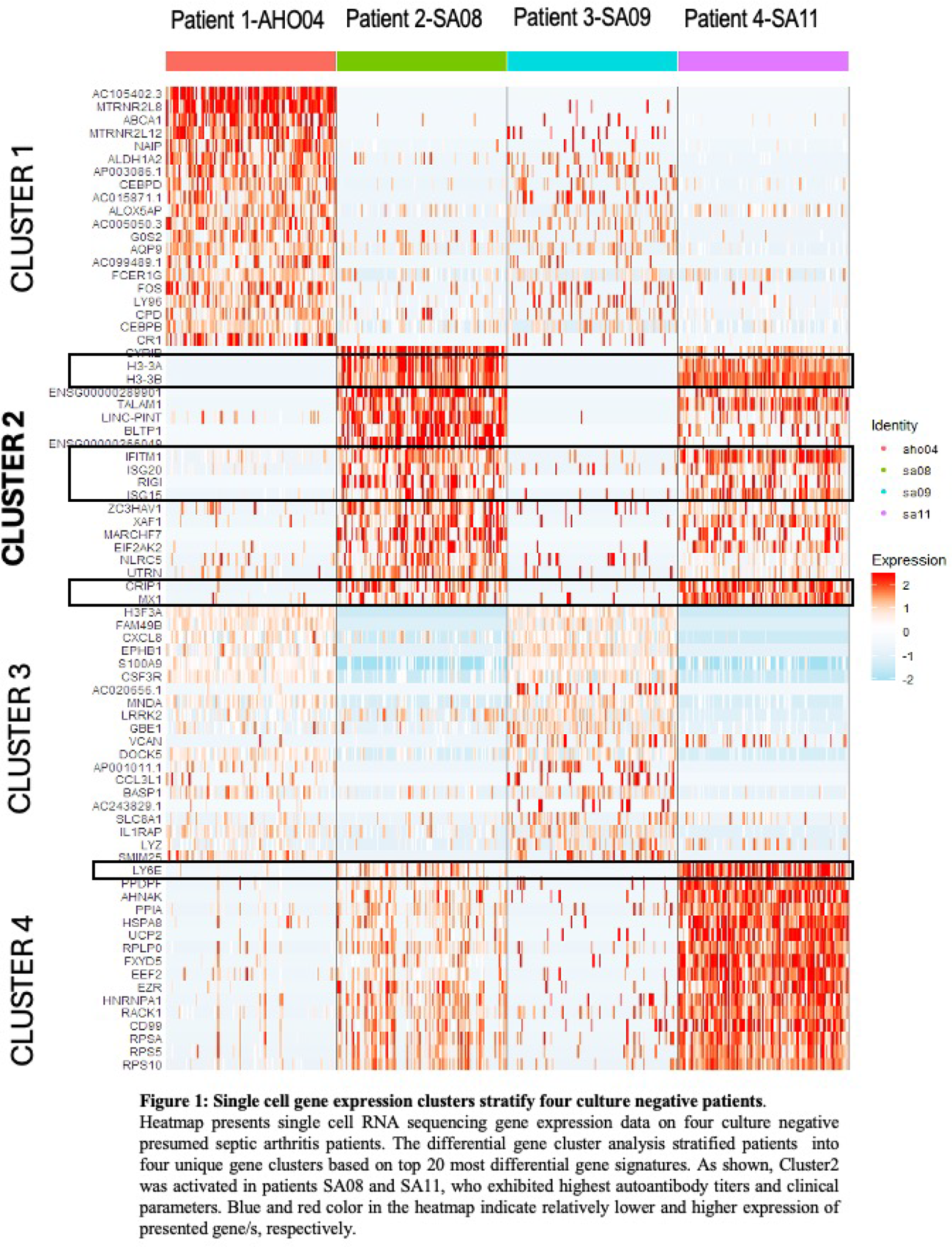
Single cell gene expression clusters stratify four culture negative patients.
Heatmap presents single cell RNA sequencing gene expression data on four culture negative presumed septic arthritis patients. The differential gene cluster analysis stratified patients into four unique gene clusters based on top 20 most differential gene signatures. As shown, Cluster2 was activated in patients SA08 and SA11, who exhibited highest autoantibody titers and clinical parameters. Blue and red color in the heatmap indicate relatively lower and higher expression of presented gene/s, respectively.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.