fetching data ... 
Background: Patients with rheumatoid arthritis (RA) face an elevated risk of herpes zoster (HZ) due to the use of immunomodulating treatments. HZ is preventable via vaccination, and the adjuvanted recombinant herpes zoster vaccine has demonstrated efficacy and safety in this population, both in randomised trials and in real-world data analyses [1,2]. Still, few patients with RA are vaccinated [3]. The lack of cost-effectiveness analyses has been cited as one reason for the low uptake [4]. Hence, we the aim of this study is to fill this evidence gap.
Objectives: To assess the cost-effectiveness of the adjuvanted recombinant herpes zoster vaccine in patients aged 50 years old with rheumatoid arthritis.
Methods: We developed a decision analytic Markov model, comparing a cohort of 10 000 RA patients vaccinated against herpes zoster with an unvaccinated cohort (standard of care, SoC). The cohorts are aged 50 years old and they are evaluated over a lifetime horizon, applying an extended healthcare perspective on costs. The model records episodes of herpes zoster and the associated complication post herpetic neuralgia (PHN), and their impact on health-related quality of life and healthcare costs. Health effects and costs were discounted with a factor of 4% per annum. The model is populated with information from published peer-reviewed literature on vaccine effectiveness, epidemiological parameters, and health related quality of life, while resource use and unit prices are based on literature, clinical expertise and publicly available sources. Differences in quality adjusted life years (QALYs) and cost between the two cohorts are used to calculate an incremental cost-effectiveness ratio (ICER), expressed as EUR per QALY, an indicator of cost-effectiveness. Vaccination is considered cost-effective if the ICER is below a cost-effectiveness threshold of EUR 24,000 per QALY. We performed one way sensitivity analyses presented as a tornado diagram and probabilistic sensitivity analysis presented as a cost-effectiveness scatter plot.
Results: Vaccinating 10,000 RA patients, led to 2,550 fewer cases of HZ and a reduction of 1,303 cases of PHN, this resulted in a health gain of 0.016 QALYs per vaccinated patient. The additional cost per patient vaccinated was EUR 185. Together, these effects gave an ICER of EUR 11,562 per QALY gained.
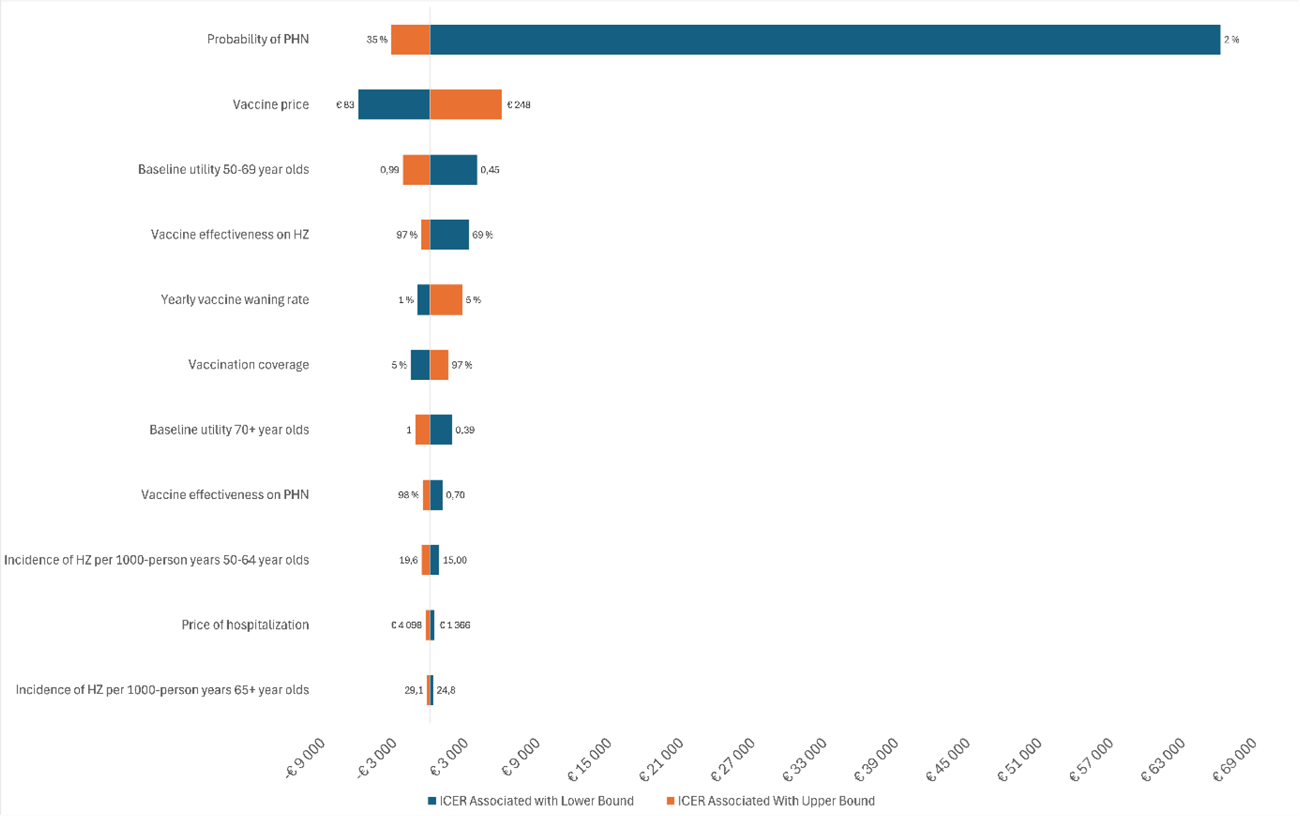
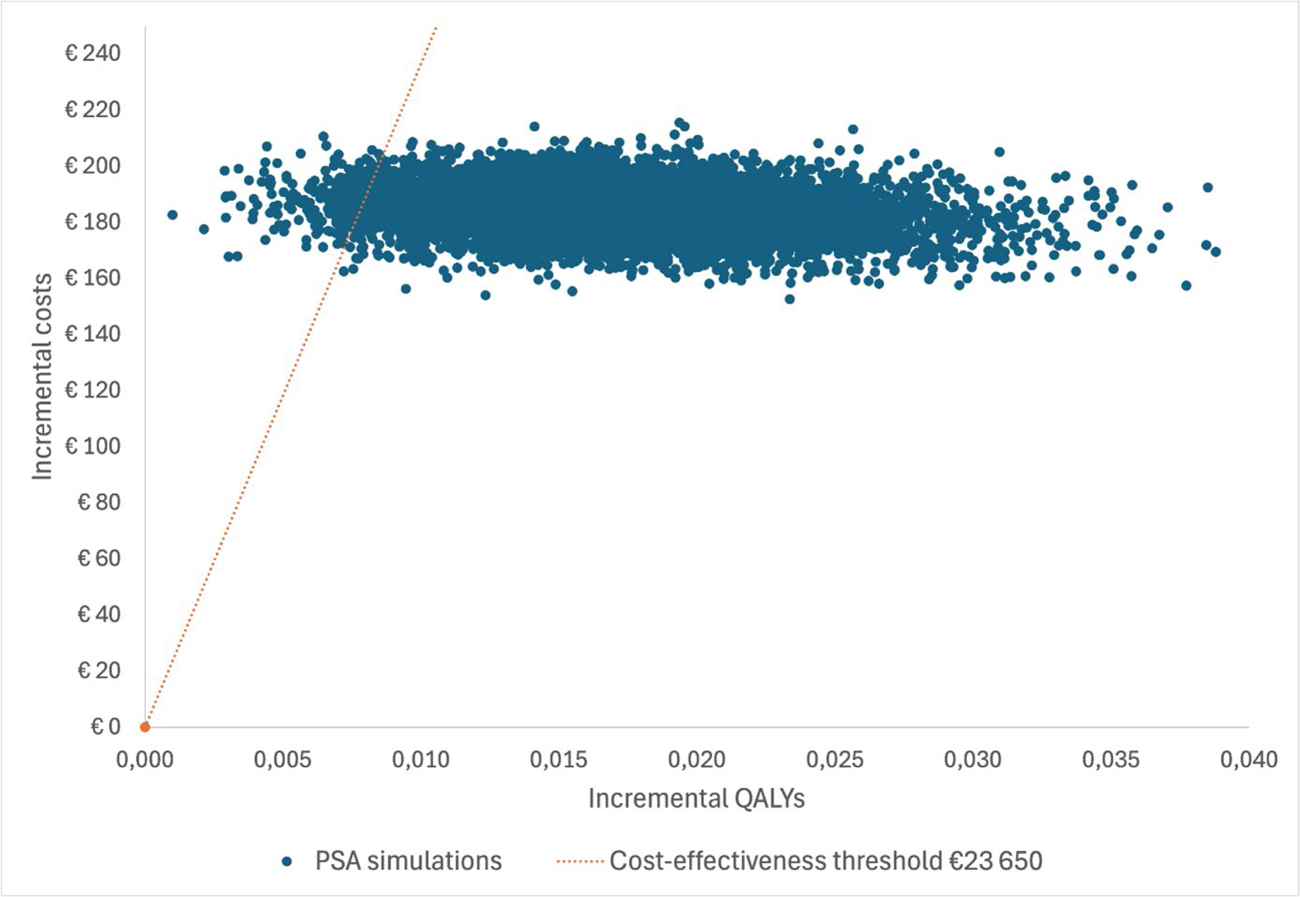
The tornado diagram revealed that the ICER was very sensitive to the probability of developing PHN (Figure 1): for the lower value of 2%, the ICER increases to EUR 77,389 per QALY, while for the upper value of 35%, the ICER drops to EUR 7,973 per QALY. The ICER is also sensitive to vaccine effectiveness against HZ and price. In the probabilistic sensitivity analysis, vaccination generated better health and higher costs, with a 98% probability of being considered cost effective at the assumed threshold of EUR 24,000 per QALY. Results plotted on the cost-effectiveness plane shows that all probabilistic simulations showed better health and higher costs, with a higher uncertainty in the size of the health gain than in the costs (Figure 2).
Conclusions: Vaccination against herpes zoster in RA patients lead to better health outcomes and increased costs. Given the assumptions made, vaccination is very likely to be considered a cost-effective alternative.
Tornado diagram over one-way sensitivity analyses
Cost-effectiveness scatter plot
REFERENCES: [1] Christensen IE, Lillegraven S, Sexton J, Kvien TK, Uhlig T, Provan SA. Longitudinal risk of serious infections in patients with inflammatory arthritis on immunomodulating therapy compared to controls. Rheumatol Adv Pract. 2025;9(1):rkaf017.
[2] Dagnew AF, Rausch D, Hervé C, Zahaf T, Levin MJ, Schuind A. Efficacy and serious adverse events profile of the adjuvanted recombinant zoster vaccine in adults with pre-existing potential immune-mediated diseases: a pooled post hoc analysis on two parallel randomized trials. Rheumatology (Oxford). 2021;60(3):1226-33.
[3] Rayens E, Sy LS, Qian L, Wu J, Ackerson BK, Luo Y, et al. Effectiveness and safety of the recombinant zoster vaccine in individuals ≥50 years of age with rheumatoid arthritis: a matched cohort and self-controlled case series study. Ann Rheum Dis. 2025.
[4] Wong PK, O’Sullivan M, Deng L. POS1242 Influenza, pneumococcal and herpes zoster vaccination coverage in Australiam patients commencing a biologic or tareted synthetic disease modifying anti-rheumatic drug for inflammatory arthtitis. Annals of the Rheumatic Diseases. 2025;84:1297.
[5] Pier M, Wolbink G, Boekel L. Time to talk to adults with rheumatic diseases about herpes zoster vaccination. Lancet Rheumatol. 2024;6(4):e247-e51.
Acknowledgments: NIL.
Disclosure of Interests: Gunhild Hagen Employed by Pfizer from 2015-2018, Anna Kristine Opheim: None declared, Joakim Ovrebo: None declared, Eline Aas: None declared, Sella Aarrestad Provan: None declared.