fetching data ... 
Background: Antiphospholipid antibodies (aPL) are central to the pathogenesis of thrombotic antiphospholipid syndrome (APS) [1]. Emerging evidence suggests that aPL negativization may have prognostic relevance by reducing the risk of recurrent thrombosis [2]. It is unclear whether the immunopathogenic effects associated with aPL persistence are reversible once aPL become undetectable, namely the dysregulation of germinal-centre T cells sustaining aPL production.
Objectives: To characterize the T-cell dysregulation and altered thrombin generation associated with aPL persistence in APS, and to test whether aPL negativization restores immune and thrombogenic balance.
Methods: We conducted a cross-sectional study including 75 patients with primary thrombotic APS (ACR/EULAR criteria) followed at a dedicated APS clinic at Hospital Santa Maria, Lisbon, Portugal, and 70 age- and sex-matched healthy donors (HD), that served as controls. Clinical and laboratory data were collected at baseline. Patients were stratified according to baseline aPL profile (lupus anticoagulant [LA]; IgM/IgG anti-cardiolipin [aCL], anti-b2-glycoprotein [aβ2GPI], anti-phosphatidylserine/prothrombin complex [PS/PT]; and IgG anti-Domain-1 of β2GPI [D1-β2GPI]) into two groups: aPL-positive (aPL+, n=51), persistently positive for at least one aPL; and aPL-negative (aPL-, n=11), currently negative for all aPL after previous positivity. T-cell immunophenotyping was performed by flow cytometry using cryopreserved peripheral blood mononuclear cells. Thrombin generation assay (TGA) was carried out using plasma from 34 APS patients (17 aPL+) and 31 disease-control (DC) participants. Owing to limited plasma availability, APS patients included in TGA analysis were recruited both from our institution and from the San Giovanni Bosco Hub Hospital, Turin, Italy, where TGA measurements were performed. The DC group consisted exclusively of patients followed at the latter centre for long-term vitamin K antagonist (VKA) therapy due to non-APS indications. All participants included in the TGA analysis were receiving VKA treatment with a target international normalized ratio of 2–3. Giving the small and unequal group sizes, pairwise comparisons were performed using the Mann-Whitney U test.
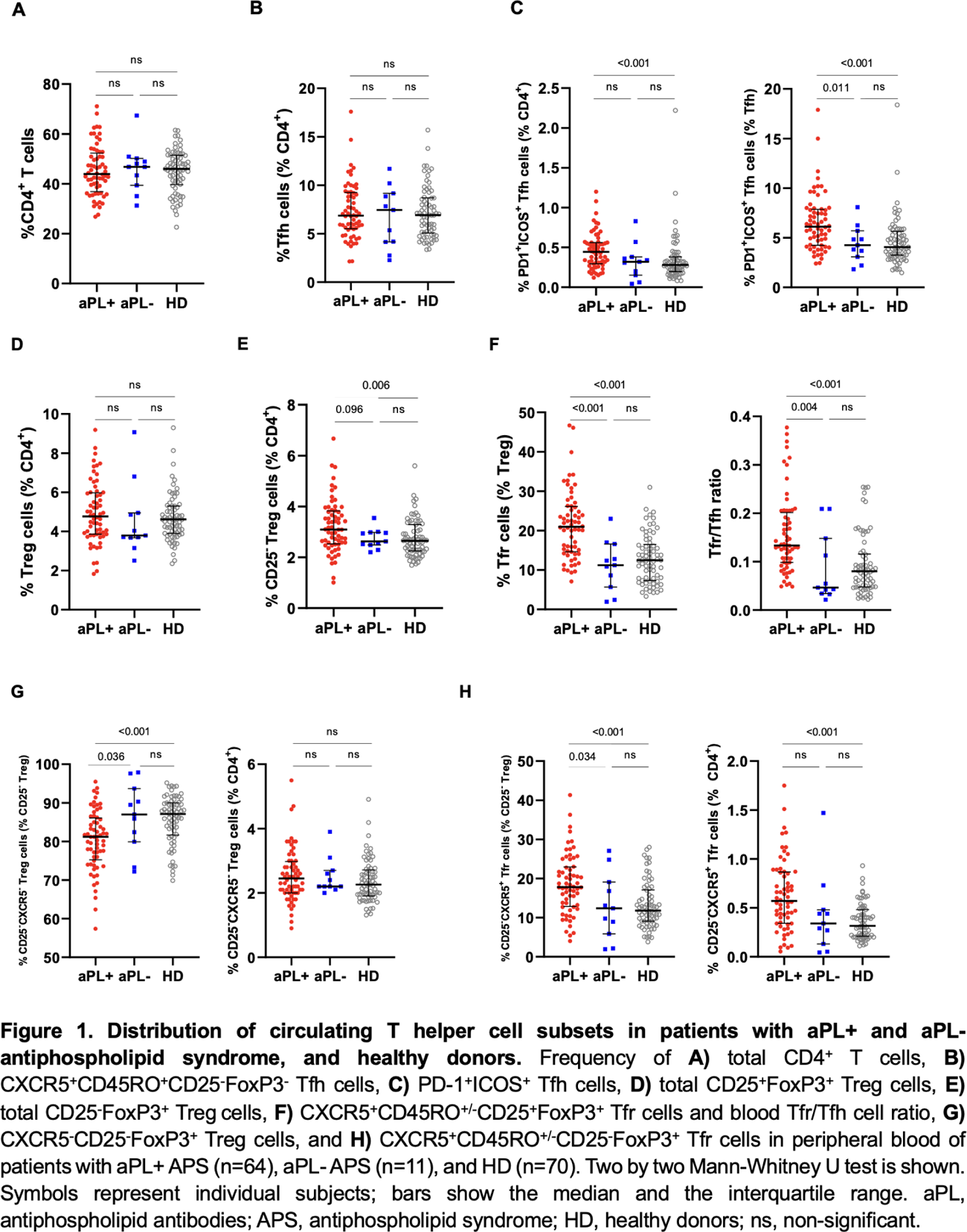
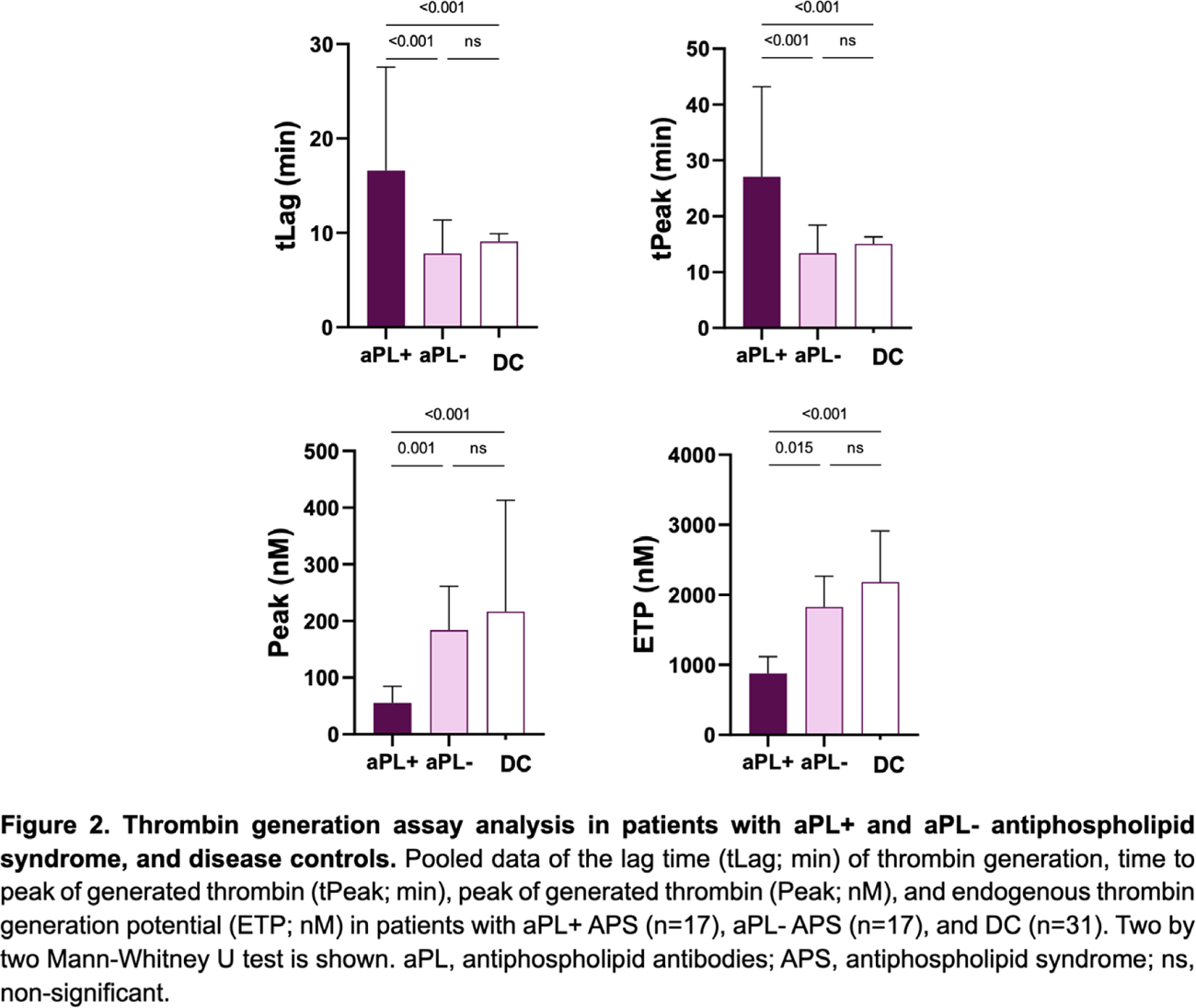
Results: Most APS patients were women (n=42, 62.7%), with a median age of 50 years and a median follow-up of 4 years. Arterial thrombosis was the most frequent first manifestation (61.3%). Prevalence of aPL at baseline was: LA (30.7%); aCL (36.0%); aβ2GPI (38.7%), anti-PS/PT (37.3%), and anti-D1-β2GPI (26.7%). Demographic and clinical characteristics were comparable between APS groups. While the total CD4 + T cells and global T follicular helper (Tfh) cells frequencies did not differ among aPL+ APS, aPL- APS, and HD ( Figure 1A and B ), the activated Tfh cells (defined as PD-1 + ICOS + ) were expanded only among aPL+ APS compared with aPL- APS and HD ( Figure 1C ). Within regulatory compartment, conventional CD25 + FoxP3 + Treg cells were similarly distributed across groups ( Figure 1D ), while the total CD25 − FoxP3 + Tregs were increased in aPL+ APS compared with HD and aPL- APS patients, even though without reaching a statistically significant difference with the latter ( Figure 1E ). Within CD25 + Treg cells, aPL+ APS patients displayed a significant expansion of circulating T follicular regulatory (Tfr) cells, resulting in an elevated Tfr/Tfh ratio compared to HD ( Figure 1F ); this was not observed in aPL- APS patients. A similar pattern emerged among CD25 − Treg cells, where stratification into CXCR5 − CD25 − Tregs (true CD25 − Tregs) and CXCR5 + CD25 − follicular counterparts (CD25 − Tfr cells) showed that the overall increase in total CD25 − Tregs in aPL+ APS was entirely driven by the follicular subset, with aPL- APS showing levels comparable to HD ( Figure 1G and H ). In TGA ( Figure 2 ), aPL+ APS exhibited a prolonged lag time and time-to-peak of thrombin generated compared to DC, together with reduced peak thrombin and endogenous thrombin potential. All parameters in aPL- APS overlapped closely with DC values, indicating normalization of thrombin-generation capacity upon aPL disappearance.
Conclusions: APS shows a preferential disruption of follicular immune regulation, with expansion of activated Tfh cells and Tfr subsets, supporting a broad dysregulation of the GC response encompassing both effector and regulatory arms. These abnormalities, together with parallel impaired thrombin generation, normalize in patients who become aPL-. This finding supports the view of APS as a dynamic and reversible pathophysiological state, in which the restoration of the germinal centre autoimmune response resolves aPL production, thereby enabling normalization of the thrombotic potential. Elucidating the immunological mechanisms underlying aPL negativization may therefore have therapeutical implications.
REFERENCES: [1] Knight JS, Branch DW, Ortel TL. Antiphospholipid syndrome: advances in diagnosis, pathogenesis, and management. BMJ. 2023 Feb 27;380:e069717.
[2] Gaspar P, Cruz-Machado AR, Abrantes AM, Costa F, Parreira I, Lopes AR, et al. Loss of antiphospholipid antibody positivity decreases the risk of recurrent thrombosis in thrombotic antiphospholipid syndrome. Rheumatology. 2025 Dec 14;keaf679. doi: 10.1093/rheumatology/keaf679.
Acknowledgments: NIL.
Disclosure of Interests: None declared.