fetching data ... 
Background: Axial spondyloarthritis (AxSpA) is a chronic immune-mediated inflammatory disease affecting approximately 0·5% of the general population [1].
Biological sex is increasingly recognised as an important factor in determining the clinical presentation and treatment response in AxSpA [2], with men more likely to achieve clinically important improvement upon TNF inhibitor initiation than women [3]. Higher Th17 T cell frequencies have also been described previously in men with AxSpA [4].
Objectives: We compared the immunologic signature in the blood of female and male patients with active AxSpA and asked if sexual dimorphism is associated with response to biological therapy.
Methods: Peripheral blood mononuclear cells were obtained pre- and post-treatment for 51 AxSpA patients, 25 AxSpA patients initiating TNF inhibition, and 26 AxSpA patients participating in the first in-disease phase II clinical trial of a GM-CSF neutralising monoclonal antibody (namilumab) in AxSpA (NAMASTE trial [5]), together with 20 age and sex-matched healthy controls. Participants aged 18–75 years with AxSpA meeting the Assessment in SpondyloArthritis international Society (ASAS) diagnostic criteria and who had active disease as defined by Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) [6] and spinal pain component of ≥4, were eligible. Patients’ informed written consent was obtained under either the NAMASTE study protocol (approved by the Oxford A research ethics committee (18/SC/0241) and registered with EudraCT (2018–000176–15) and ClinicalTrials.gov (NCT03622658)) or the “Immune function in Inflammatory Arthritis (IFIA)” study (REC06/Q1606/139). Myeloid and T cell populations were enumerated by a 41-marker high dimensional Cytometry by Time of Flight (CyTOF) panel [7].
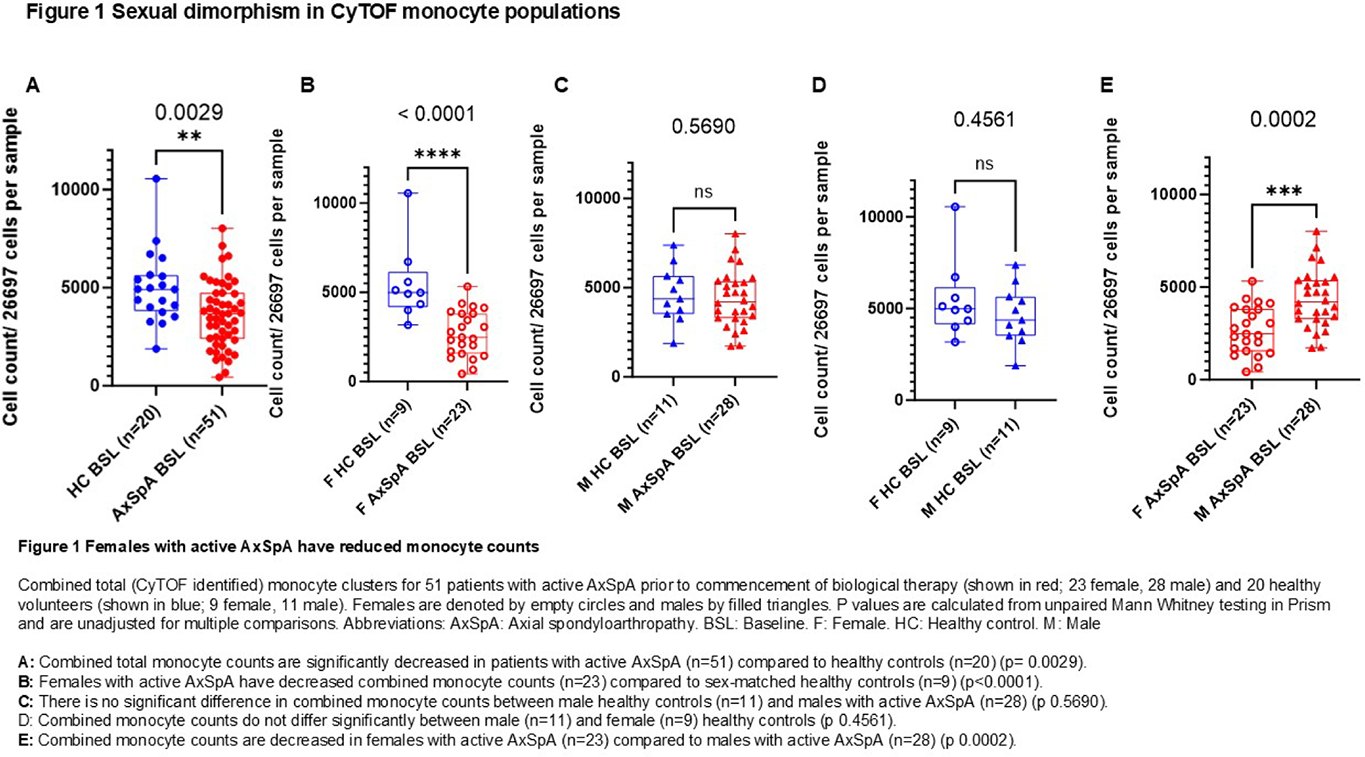
Results: Data was analysed for 51 patients with active AxSpA and 20 healthy controls. Unbiased CyTOF immunophenotyping delineated 35 myeloid and lymphoid cell populations, including six monocyte populations. These were, in diminishing frequency, CD141low CD66b- (classical) monocytes, CD141high CD66b- (classical) monocytes, CD9- CD36- (nonclassical) monocytes, CD9+ CD36+ (nonclassical) monocytes, CD141-CD14low intermediate-like monocytes and CD11b+ CD66b+ (classical) monocytes. Combined analysis of the six identified monocyte populations shows that total monocyte counts were significantly decreased in patients with active AxSpA (n=51) compared to healthy controls (n=20) (p= 0.0029, Figure 1A). Sex-stratified analysis shows that this is due to decreased combined monocyte counts in women with active AxSpA (n=23) compared to sex-matched healthy controls (n=9) (p<0.0001, Figure 1B) and men with active AxSpA (n=28) (p 0.0002, Figure 1E). Combined monocyte counts do not differ between male AxSpA patients (n=28) and male healthy controls (n=11) (p 0.5690, Figure 1C) and between female and male healthy controls (n=20) (p 0.4561, Figure 1D). Cluster stratified analysis shows that women with active AxSpA (n=23) have reduced CD141low CD66b- (classical) monocytes (p 0.0042), CD141high CD66b- (classical) monocytes (p 0.0142) and CD9+ CD36+ (nonclassical) monocyte counts (p 0.0047) compared to sex-matched healthy controls (n=9). This is not the case for men. By contrast, CD11b+ CD66b+ (classical) monocyte counts are elevated in male patients with active AxSpA (n=27) compared to male healthy controls (n=11) (p 0.0301) and female patients with active AxSpA (n=23) (p 0.0647). CD11b+ CD66b+ (classical) monocytes express cell surface markers also expressed on low density neutrophils (LDNs); with LDN counts also being increased in men with active AxSpA (n=28) compared to sex matched healthy controls (n=11) (p 0.0396). In pre to post treatment comparisons, CD141low CD66b- (classical) and CD9+ CD36+ (nonclassical) monocyte populations tend to increase under GM-CSF and TNFα inhibition in female AxSpA patients. This reaches nominal significance for CD141low CD66b- (classical) monocytes in the ten women treated with namilumab (p 0.0195); and for CD9+ CD36+ (nonclassical) monocytes in the twelve women treated with TNF inhibition (p 0.0342).
Conclusions: We observe significant sexual dimorphism in monocyte populations in patients with active AxSpA. Whilst this needs independent verification our work highlights the importance of sex-stratified data analysis in the study of immunobiology in AxSpA and contributes to the evolving understanding of clinically observed differences in presentation and treatment response in men and women with AxSpA.
REFERENCES: [1] Raine, C. and A. Keat, Axial spondyloarthritis. Medicine, 2014. 42 (5): p. 251-256.
[2] Marzo-Ortega, H., et al., The impact of gender and sex on diagnosis, treatment outcomes and health-related quality of life in patients with axial spondyloarthritis. Clinical Rheumatology, 2022. 41 (11): p. 3573-3581.
[3] Hellamand, P., et al., Sex differences in the effectiveness of first-line tumour necrosis factor inhibitors in axial spondyloarthritis: results from the EuroSpA Research Collaboration Network. RMD Open, 2023. 9 (4): p. e003325.
[4] Gracey, E., et al., Sexual Dimorphism in the Th17 Signature of Ankylosing Spondylitis. Arthritis Rheumatol, 2016. 68 (3): p. 679-89.
[5] Worth, C., et al., Granulocyte-macrophage colony-stimulating factor neutralisation in patients with axial spondyloarthritis in the UK (NAMASTE): a randomised, double-blind, placebo-controlled, phase 2 trial. The Lancet Rheumatology, 2024. 6 (8): p. e537-e545.
[6] Garrett, S., et al., A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol, 1994. 21 (12): p. 2286-91.
[7] Nowicka, M., et al., CyTOF workflow: differential discovery in high-throughput high-dimensional cytometry datasets. F1000Res, 2017. 6 : p. 748.
Acknowledgments: NIL.
Disclosure of Interests: Claudia Worth Speaker fees for Novartis, 3-month research funding from Izana Biosciences, Feng Liu: None declared, David Ahern: None declared, Antoni Chan Speaker for Novartis, UCB, Abbvie, Medac, Frank Penkava: None declared, Liye Chen: None declared, Nicole Yager: None declared, Anna Ridley: None declared, Hussein Al Mossawi GSK, UCB Pharma, Previous full time employee of AstraZeneca and UCB, Paul Bowness Research funding from GSK.