fetching data ... 
Background: Psoriatic arthritis (PsA) is a heterogeneous immune-mediated inflammatory disease with variable clinical response to systemic therapies. While biologic and conventional disease-modifying antirheumatic drugs (DMARDs) are effective in many patients, predictors of treatment response remain poorly defined. Circulating immune-cell phenotypes may reflect disease biology and treatment responsiveness, but comprehensive longitudinal immunoprofiling linked to validated clinical outcomes in real-world PsA cohorts is limited.
Objectives: To identify peripheral immune-cell signatures associated with clinical improvement and remission in PsA patients initiating new systemic therapy, using integrated flow cytometry and single-cell RNA sequencing (scRNA-seq).
Methods: COLIPSO is a prospective, multicentre observational cohort of patients with psoriatic disease initiating new systemic therapy.
High-dimensional spectral flow cytometry was performed to quantify prespecified CD4 + T-cell subsets, including regulatory T cells (Treg), activated CD4 + effector cells, Th17, Th22, Th9, MAIT cells and other canonical populations. Associations between immune-cell abundances at baseline and longitudinal clinical outcomes (including change in Disease Activity in Psoriatic Arthritis (DAPSA), swollen joint count (SJC), body surface area (BSA), Psoriatic Arthritis Disease Activity Score (PASDAS), iron-corrected T1 (cT1) and liver fat content were assessed using Bayesian linear mixed-effects models with patient-level random intercepts, adjusting for age, sex, BMI, sample processing batch, and treatment group. Interaction terms between immune-cell abundance and timepoint were used to evaluate whether baseline immune states predicted clinical change. Single-cell RNA sequencing was performed on PBMCs from a subset of patients. Cells were clustered using Leiden algorithms and annotated using marker-based and automated classification. Pseudobulk differential gene expression analyses were conducted using mixed-effects models, comparing patients achieving Minimal Disease Activity (MDA) at follow-up (“remission”) versus non-remission, with subject included as a random effect.
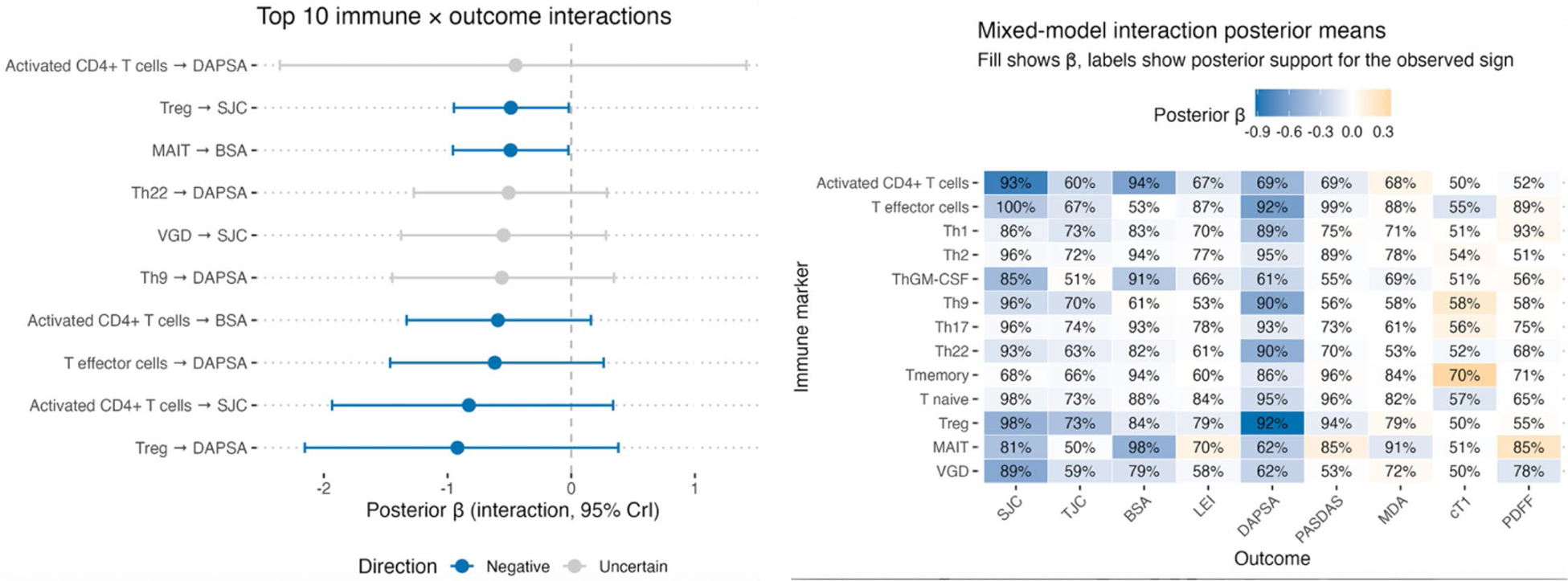
Results: Seventeen PsA patients were included (median age 52 years; 10 female), with paired baseline and ~24-week PBMC samples. Twelve patients (71%) achieved MDA at follow-up. Treatments included csDMARDs (n=4), TNF inhibitors (n=8) and IL-17 inhibitors (n=5). Higher frequencies of Treg cells, activated CD4 + effector T cells, Th22 cells and Th9 cells at baseline were associated with reductions in DAPSA, BSA and swollen joint counts. (Figure 1) Posterior probabilities supporting a negative interaction (greater immune abundance associated with greater improvement) exceeded 90% for multiple CD4 + lineages across joint-related outcomes. The strongest and most credible immunophenotype–outcome associations were with ΔDAPSA, ΔSJC and ΔBSA, with relatively weaker or inconsistent associations for other clinical domains. Innate-like populations showed fewer robust associations; however, a weak signal was observed between MAIT-cell abundance and longitudinal clinical change.
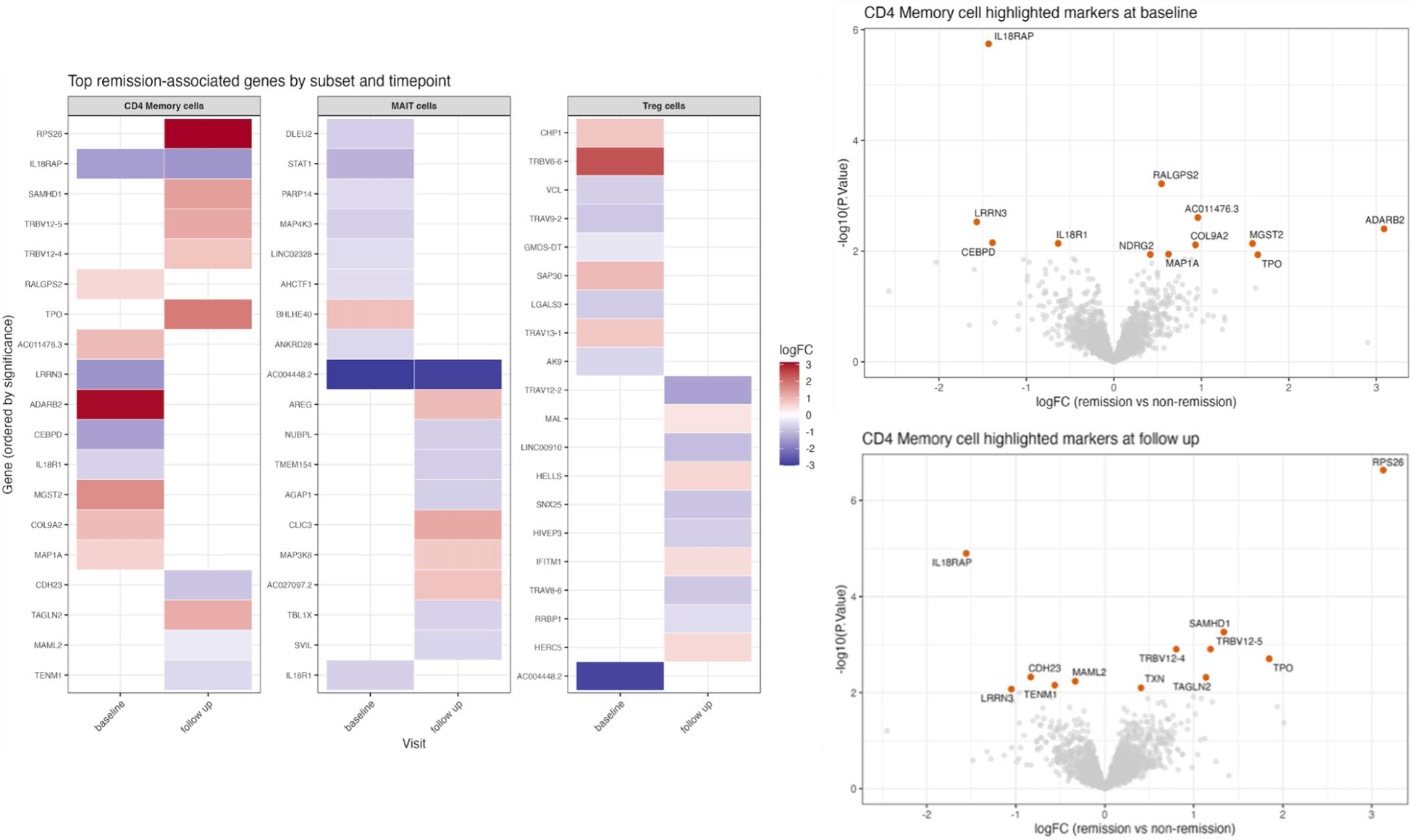
Single-cell RNA sequencing revealed transcriptional differences at baseline associated with remission status when all treatment groups were pooled, most prominently within CD4 + memory T helper cells. (Figure 2) At baseline, IL18RAP expression was significantly lower in patients who subsequently achieved MDA at follow-up. At follow-up, remission was associated with marked upregulation of ribosomal gene RPS26 , and persistently low expression of IL18RAP . MAIT cell and Treg subsets showed consistent but modest trends in inflammatory signalling pathways at baseline and follow-up, without statistically significant differential expression after multiple testing correction.
Conclusions: In this prospective real-world PsA cohort, baseline T cell immunophenotype, particularly regulatory and activated CD4 + T-cell populations, were associated with subsequent improvement in joint disease activity and achievement of minimal disease activity. Flow cytometry–based mixed-effects modelling identified several adaptive immune-cell populations whose baseline abundance was associated with greater clinical improvement over follow-up. Single-cell transcriptomic analyses implicate reduced IL-18–driven inflammatory signalling in CD4 + memory T cells as a feature of clinical remission. These findings suggest that circulating immune-cell states at treatment initiation may help stratify the likelihood of clinical response, and warrant investigation in larger studies to support the development of immune-based biomarkers to guide personalised therapy in psoriatic arthritis.
(a) Posterior coefficients of the interaction between immune subset and clinical outcome measures with interaction term and 95% credible intervals; (b) Global interaction heatmap, whereby the fill colour shows the posterior coefficient for the interaction term, and the labels the posterior support for the observed sign. Blue indicates a negative direction and orange a positive direction of association. The heatmap outcome is the absolute change from baseline (T2−T1) in the original units. The mixed-effects model accounts for repeated measures via a subject random intercept.
(a) Heatmap of genes most associated with differing MDA status at follow up in CD4 + memory, MAIT and Treg cells. (b) Volcano plots of highly associated genes in CD4 + memory cells at baseline and follow-up. Volcano plot showing differential expression between remission and non-remission: x-axis is log2fold-change (logFC) from the dreamlet model, y-axis is -log10 (p-value). Points highlight the top genes by FDR.
REFERENCES: NIL.
Acknowledgments:
Disclosure of Interests: Shannon Gunawardana: None declared, Lija James: None declared, Charlie Diamond Perspectum Ltd, Anneli Andersson Perspectum Ltd, Jiaqi Li: None declared, Sinibaldo Arocha: None declared, Moustafa Attar: None declared, Hussein Al Mossawi Novartis, Pfizer, UCB, UCB, GSK, BMS, Previous Employee at UCB,
AstraZeneca, Immunocore, Abbvie, Roche, Novartis, Helena Thomaides Brears Perspectum Ltd, Laura C. Coates AbbVie, Amgen, Eli Lilly, Janssen, Novartis, Pfizer and UCB, AbbVie, Amgen, Bristol Myers Squibb, Eli Lilly, Enlivex, Janssen, Moonlake, Novartis, Oruka, Pfizer, Proximi-T, Sitryx, Takeda and UCB, Abbvie, Amgen, Janssen and UCB, Alexander Clarke: None declared.