fetching data ... 
Background: Secondary hemophagocytic syndrome (HPS) is a severe complication arising secondary to connective tissue diseases, infections, or malignancies, causing systemic inflammation and pancytopenia. Secondary HPS caused by connective tissue diseases is also termed macrophage activation syndrome (MAS), reflecting the inflammatory macrophage activation observed in this syndrome. Although MAS is a life-threatening complication of connective tissue diseases, its pathogenesis remains incompletely understood. MAS is a heterogeneous syndrome driven by different disorders and immune cells. This complexity provides a challenging field for elucidating the mechanism of these conditions.
Objectives: The objective of this study is to investigate immune cell characteristics and therapeutic candidates for MAS.
Methods: We collected human bone marrow (BM) aspiration and whole blood samples from 11 MAS patients. The patients included 2 adult Still’s disease, 1 histiocytic necrotizing lymphadenitis, 3 malignant lymphoma, 1 lung cancer, 3 viral infection, and 1 drug-induced MAS patients. We applied Seq-Well (reference 1), a portable platform of single-cell RNA sequencing (scRNA-seq), to analyze gene expressions in immune cells in BM and blood among different etiologies. We also performed in-vivo experiments by using MAS mouse model that develops hypercytokinemia, hemophagocytosis, and pancytopenia following repeated administration of oligonucleotide DNA containing unmethylated CpG sequences (CpG-DNA, reference 2) to validate the scRNA-seq analysis and identify potential therapeutic targets for MAS. Twenty-four C57BL/6 mice were divided into two groups and received intraperitoneal injections of CpG-DNA or control PBS on days 0, 2, 4, 6, and 8. As therapeutic agents, IL-1 inhibitors, IL-6 inhibitors, and IL-10-albumin fusion protein (SA-IL-10, reference 3) were administered on day 0 and 5, and their therapeutic effects were compared. Mice were euthanized on day 10, and blood and bone marrow samples were analyzed.
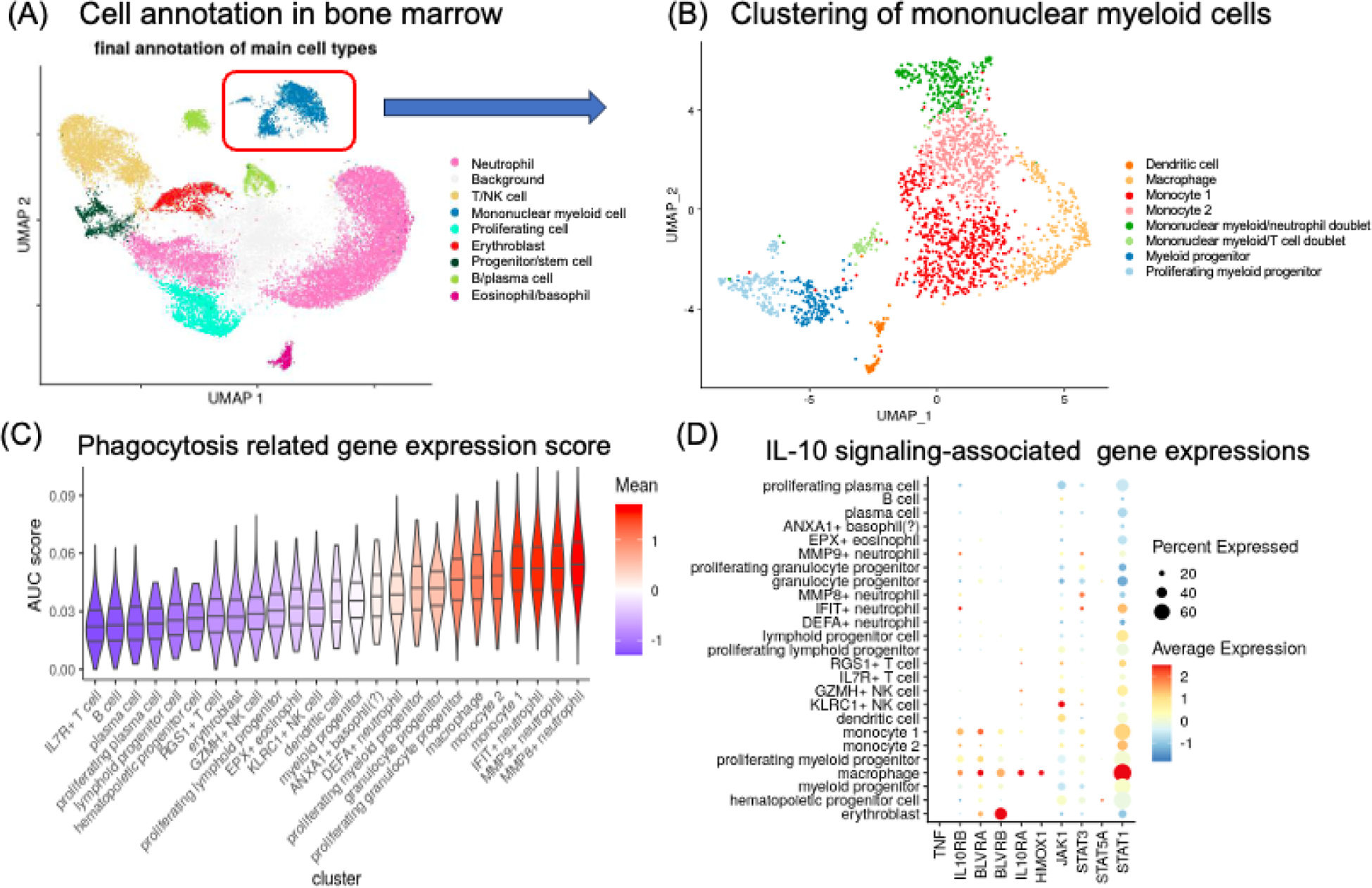
Results: In human scRNA-seq dataset, we annotated major cell types in BM of MAS patients based on their gene expressions (Figure 1A). We further classified mononuclear myeloid cells, which are thought to be important for the pathogenesis of MAS, into 9 clusters (Figure 1B). To investigate which identified cell subsets showed the strongest enrichment of phagocytosis-associated genes, we performed signature enrichment using the AUCell method (reference 4). Interestingly, the ‘monocyte 1’ population was the most highly enriched for this signature, along with macrophages in the BM dataset (Figure 1C). Further investigation revealed that monocyte 1 and macrophages expressed high levels of the interleukin 10 receptor subunit beta (IL10RB), STAT1, and the biliverdin reductase A (BLVRA, Figure 1D). In addition, macrophages also expressed the interleukin 10 receptor subunit alpha (IL10RA). These data indicated that IL-10 signaling is important for the pathogenesis of MAS.
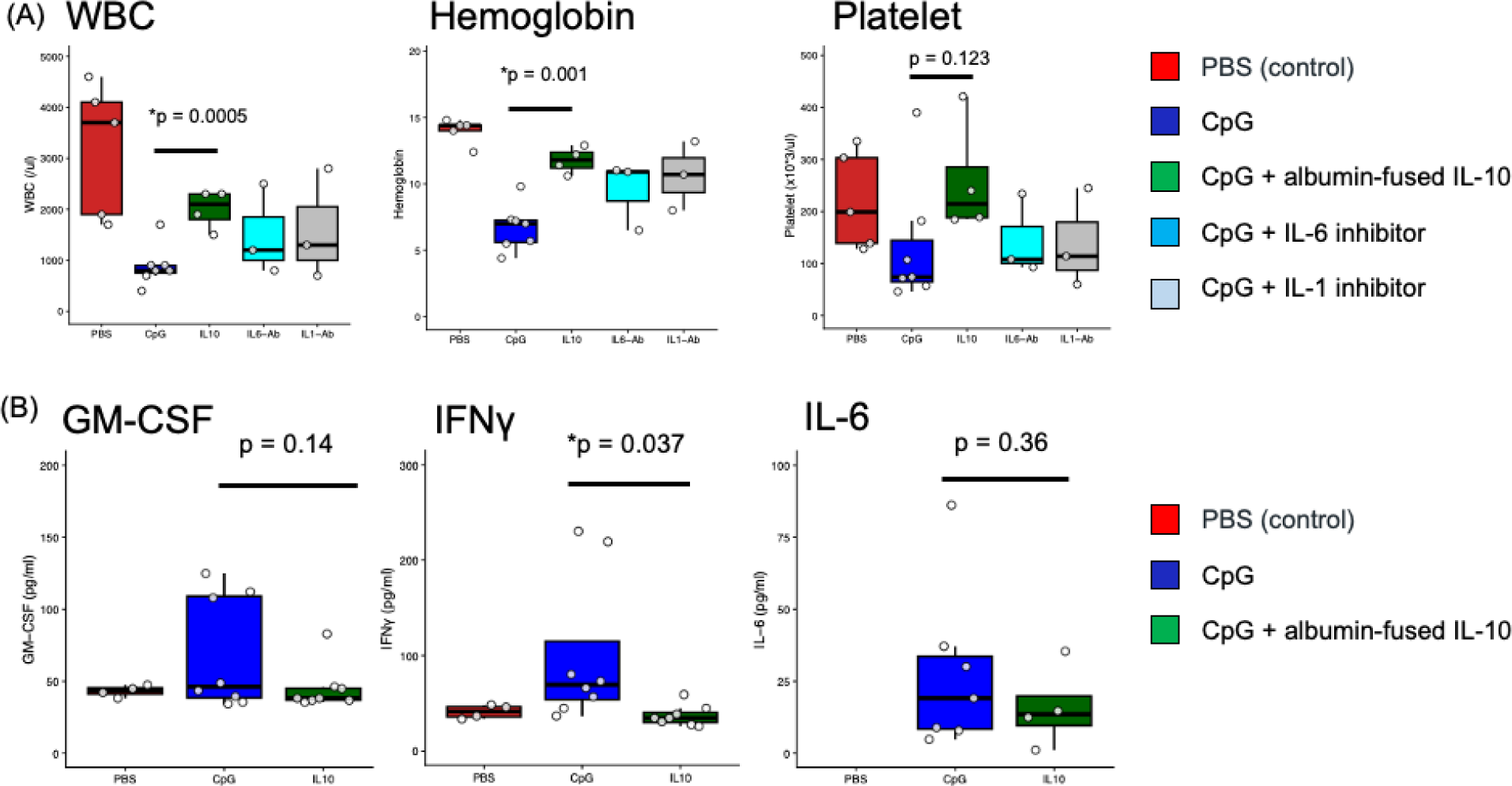
To confirm this hypothesis by in-vivo experiment, we used repeated CpG-DNA MAS model, which develops hypercytokinemia, pancytopenia with hemophagocytosis and splenomegaly. SA-IL-10 administration improved pancytopenia and splenomegaly, whereas IL-1 inhibitors and IL-6 inhibitors did not (Figure 2A). The SA-IL-10 group showed significant reductions in serum IFNγ and tendency of reduction of GM-CSF, suggesting SA-IL-10 suppresses macrophage activation by inhibiting IFNγ and GM-CSF (Figure 2B).
Conclusions: IL-10 signaling is important for MAS pathogenesis both in human and mice, suggesting it is a promising therapeutic candidate for MAS.
scRNA-seq of bone marrow cells from MAS patients.
(A) Cell type annotation of bone marrow cells from 11 MAS patients based on major gene expression. (B) Phenotypic classification of mononuclear myeloid cells based on the gene expression. (C) Enrichment of phagocytosis-gene signature in mononuclear myeloid cells and neutrophils. (D) IL-10 signaling gene signature of mononuclear myeloid cells.
Blood cell counts and cytokine levels in MAS mouse model.
(A) Blood cell counts among groups. (B) Serum cytokine levels among groups. CpG: repeated administration of oligonucleotide DNA containing unmethylated CpG sequences, IL-10: serum albumin-fused IL-10, IL6-Ab: anti-IL-6 antibody, IL1-Ab: anti-IL-1β antibody.
REFERENCES: [1] Gierahn TM et al, Seq-Well: portable, low-cost RNA sequencing of single cells at high throughput. Nat Methods 2017;14(4):395-398.
[2] Behrens EM et al, Repeated TLR9 stimulation results in macrophage activation syndrome–like disease in mice. J Clin Invest 2011; 121(6):2264-2277.
[3] Yuba E et al, Suppression of rheumatoid arthritis by enhanced lymph node trafficking of engineered interleukin-10 in murine models. Arthritis Rheumatol 2021;73(5):769-778.
[4] Aibar S et al, SCENIC: single-cell regulatory network inference and clustering. Nat Methods 2017;14(11):1083-1086.
Acknowledgments: NIL.
Disclosure of Interests: Wataru Fujii received speeking fees from Nippon Boehringer Ingelheim Co., Ltd., supported by Takeda Science Foundation, Hideaki Sofue: None declared, Eiji Yuba: None declared, Jun Ishihara: None declared, Kevin Baßler: None declared, Anna Hasegawa: None declared, Tomoka Hiyama: None declared, Sara Komatsu: None declared, Kaito Nakamura: None declared, Tomoyuki Miyao: None declared, Ayae Tanaka received speeking fees from Asahi Kasei Pharma Corporation, AbbVie GK, AstraZeneca PLC, Eisai Co., Ltd., Eli Lilly Japan K.K., KYORIN Pharmaceutical Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Chugai Pharmaceutical Co., Ltd, Nippon Boehringer Ingelheim Co., Ltd., Otsuka Pharmaceutical Co., Ltd., and Taisho Pharmaceutical Co., Ltd., Satoko Arai: None declared, Reika Maezawa: None declared, Masafumi Arima: None declared, Yutaka Kawahito received speeking fees from Asahi Kasei Pharma Co., Ltd., AbbVie Japan GK, Astellas Pharma Inc., AstraZeneca plc., Ayumi Pharmaceutical Co., Boehringer Ingelheim Japan, Inc., Bristol Myers Squibb Co., Ltd., Chugai Pharmaceutical Co., Ltd., Eisai Co., Eli Lilly Japan K.K., Ltd., Daiichi Sankyo., GlaxoSmithKline K.K., Janssen Pharmaceutical K.K., Kissei Pharmaceutical Co., Ltd., Mitsubishi-Tanabe Pharma Co., Nippon Kayaku Co., Ltd., Novartis Pharma K.K., Pfizer Japan Inc., Taisho Toyama Pharmaceutical Co., Ltd., UCB Japan Co. Ltd. and Viatris Pharmaceuticals Japan Inc., supported by Asahi KASEI Pharma Co.Ltd. and Chugai Pharmaceutical Co., Kei Ikeda received instructor fees from AbbVie GK and Eisai Co., Ltd., received speeking fees from Asahi Kasei Pharma Corporation, Astellas Pharma Inc., AbbVie GK, AstraZeneca PLC, AYUMI PharmaceuticalCorporation., Bristol-Myers Squibb K.K., Eli Lilly Japan K.K., Eisai Co., Ltd, Gilead Sciences Inc., Janssen Pharmaceutical K.K., Merck & Co., Inc., Mitsubishi Tanabe Pharma Corporation, Chugai Pharmaceutical Co., Maruho Co., Ltd, Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., and UCB Japan Co. Ltd.