fetching data ... 
Background: Health literacy, a social determinant of health, is prioritised by the World Health Organisation (WHO) for people- and community-centred care in the management of non-communicable diseases. Health literacy remains underexplored in people with rheumatic diseases. This study applies the Ophelia (Optimising Health Literacy and Access) process, an equity-driven approach, to assess health literacy strengths and challenges of people with inflammatory arthritis (IA).
Objectives: To identify distinct health literacy profiles in a national population of people with IA, using a mixed-methods approach in line with the Ophelia process, with the ultimate aim of developing tailored interventions.
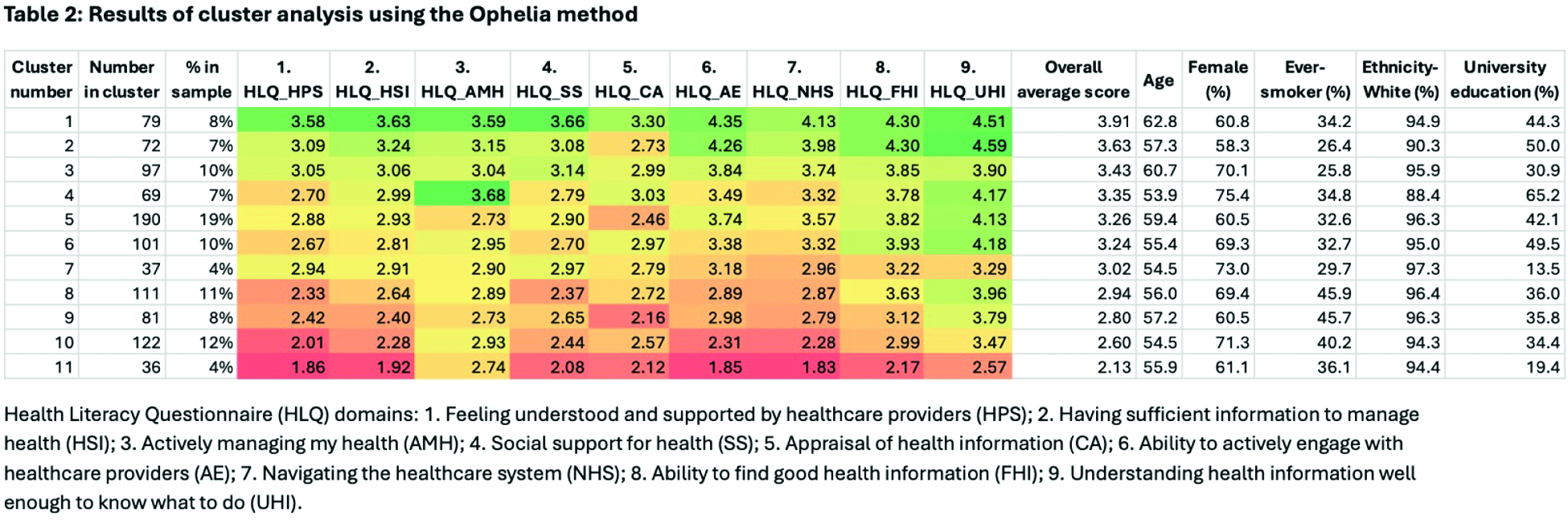
Methods: This study was undertaken in the National Early Inflammatory Arthritis Audit (NEIAA) dataset in England, an observational cohort comprising adults (≥18 years) with a diagnosis of IA recruited since 2018. Individuals with a confirmed diagnosis of IA within NEIAA were invited to complete a survey via an online platform (March-May 2024) comprising the Health Literacy Questionnaire (HLQ); Generalised Anxiety Disorder (GAD-2) and Patient Health Questionnaire (PHQ-2); Work Productivity and Activity Impairment questionnaire; socio-demographics including employment, education and marital status; current and previous treatment; and self-reported disease activity. The survey was distributed to 3300 individuals. Responses were matched with the individual’s original record within NEIAA. The HLQ comprises 44 questions across nine domains: 1. Feeling understood and supported by healthcare providers; 2. Having sufficient information to manage health; 3. Actively managing my health; 4. Social support for health; 5. Appraisal of health information; 6. Ability to actively engage with healthcare providers; 7. Navigating the healthcare system; 8. Ability to find good health information; 9. Understanding health information well enough to know what to do. Domains 1 to 5 use a 4-point Likert-type response scale; domains 6 to 9 use a 5-point scale. Higher scores indicate higher health literacy. HLQ domain scores were analysed using hierarchical cluster analysis with Ward’s method to identify subgroups with distinct multidimensional health literacy profiles. Plausible cluster solutions were identified using standard statistical criteria, after which the final solution was selected by balancing statistical information, interpretability of HLQ profiles and equity considerations, with preference given to solutions that avoided masking smaller but potentially vulnerable groups. Clusters, ordered from highest to lowest average total, were interpreted based on HLQ score patterns alongside sociodemographic and clinical data.
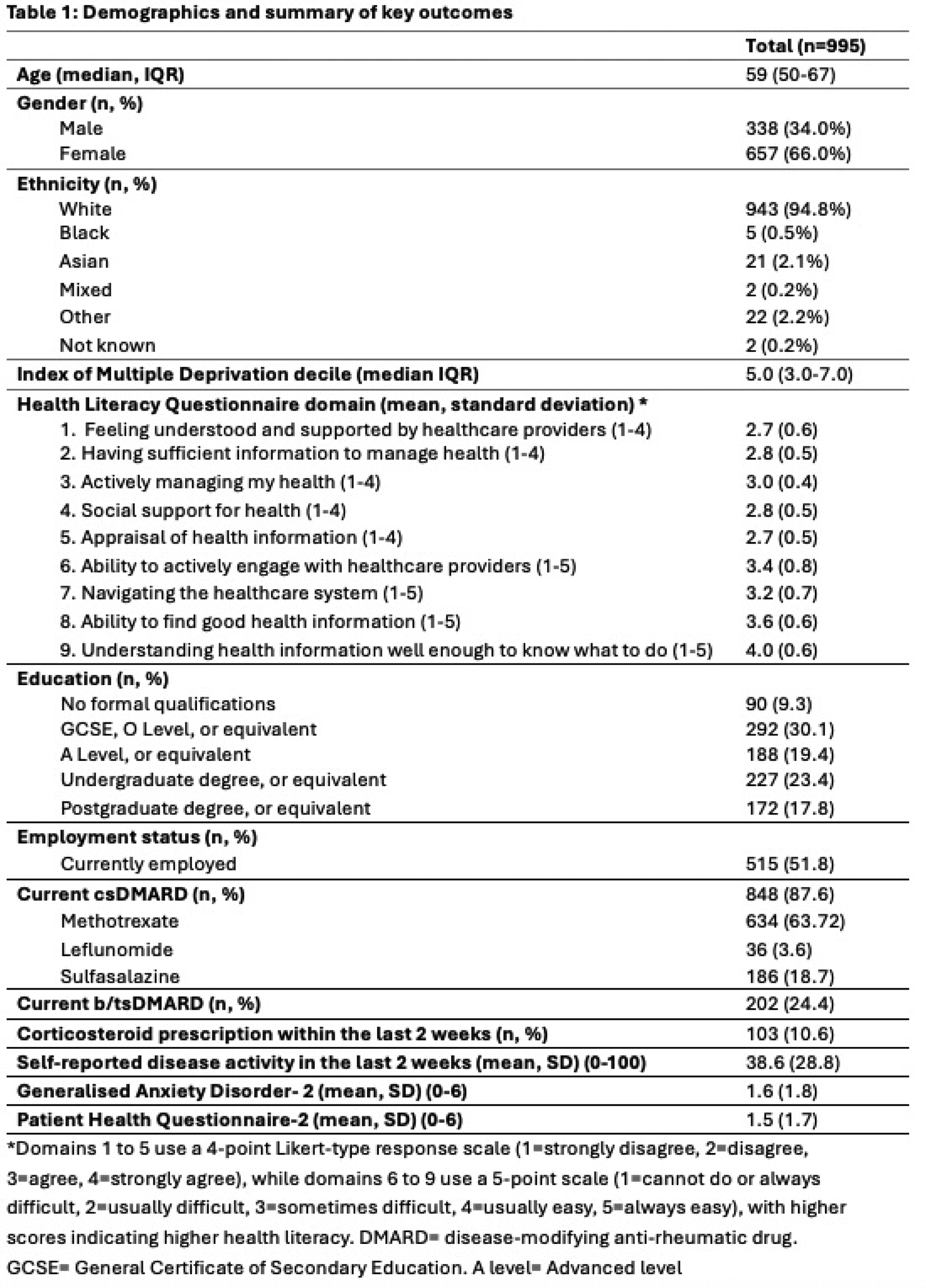
Results: In total, 995 individuals with IA responded and were included for analysis. 66% were female with a median age of 59 years (IQR 50-67); demographics are summarised in Table 1. Ultimately, an 11-cluster solution was deemed optimal, as it provided well-differentiated, interpretable multidimensional health literacy profiles with minimal within-cluster heterogeneity, while retaining sufficient granularity to avoid masking meaningful variation in health literacy strengths and challenges across subpopulations (Table 2). Cluster 5 was the largest cluster (19%) and reported having sufficient information (2.9) and generally understood information well (4.1), but appraising information was a challenge (2.5). Cluster 1 (8% of sample) had the highest health literacy scores across all domains, especially having sufficient information to manage their health, social support and understanding health information. This cluster had the highest mean age (63 years). Absenteeism and presenteeism were relatively low (3% and 22 respectively). Mean PHQ-2 and GAD-2 scores were 0.8 and 0.9 respectively (lowest scores overall). Self-reported disease activity was 29/100 (second lowest after Cluster 2). In contrast, Cluster 11 (4% of sample) had the lowest health literacy scores overall, aside from actively managing their health (2.7), indicating a strength in this area despite health literacy challenges across most domains. Cluster 11 had the second lowest university attendance (19%) and highest absenteeism (17%) of all clusters. Mean self-reported disease activity (63/100), as well as PHQ-2 and GAD-2 scores (2.7 and 2.8 respectively, indicating high depression and anxiety), were also highest in this cluster. Cluster 10, a large group (12% of sample), generally understood health information well, but had challenges in feeling supported by health professionals, actively engaging with healthcare providers, and navigating the healthcare system. This cluster had the second highest PHQ-2 and GAD-2 scores, absenteeism rates and self-reported disease activity. Cluster 4 (7% of sample) took time to manage their own health but did not feel supported by health professionals and found navigating the healthcare system difficult. This cluster had the highest proportion of people completing university (65%). The lowest proportion of people completing university was in Cluster 7 (14%), which had moderate-low scores across all HLQ domains, including challenges in understanding health information.
Conclusions: This Ophelia-informed analysis in a national cohort of people with IA identified 11 distinct health literacy profiles, highlighting substantial heterogeneity in health literacy strengths and challenges. This is the largest and most comprehensive analysis of this sort in a rheumatic disease cohort to date. The findings demonstrate that reliance on an average health literacy score alone risks obscuring smaller but potentially vulnerable groups and related socioeconomic and clinical factors, and health literacy is not directly related to one factor alone, such as education or work status. Results will be used to co-develop targeted, system-level interventions, applying an equity-driven approach, to improve access, communication and care, in line with WHO recommendations.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.