fetching data ... 
Background: Familial Mediterranean Fever (FMF) is an autoinflammatory disease characterized by recurrent, self-limited attacks of fever and serositis. Aging is associated with changes in immune system function, particularly within the innate immune response, resulting in altered inflammatory reactions. However, data regarding the clinical behavior, attack characteristics, and disease severity of FMF in older patients are limited. Understanding FMF in later life may provide insights into disease evolution and management across the lifespan.
Objectives: The aim of this study was to evaluate the clinical phenotype, disease activity, and long-term disease course of FMF in patients aged 50 years and older.
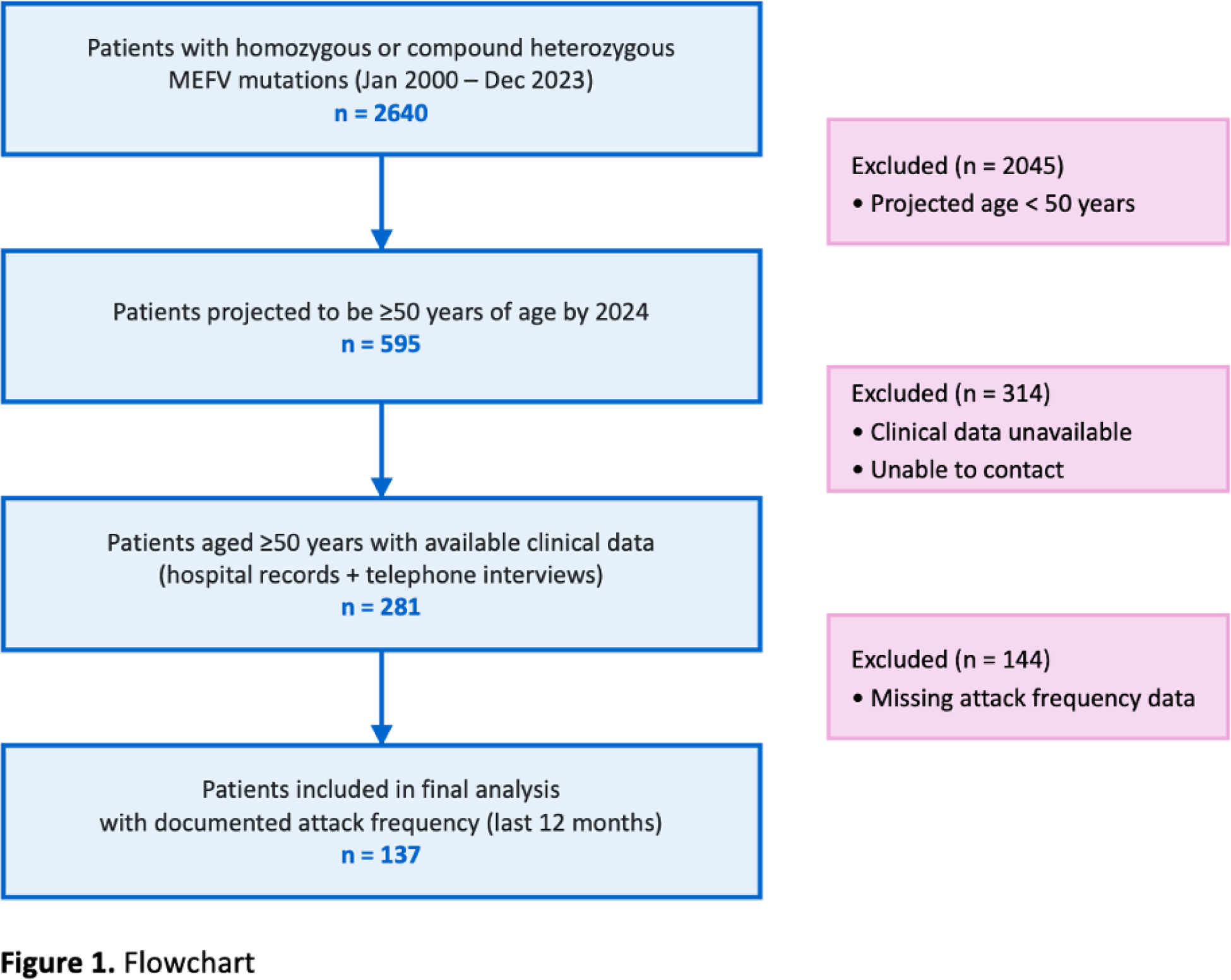
Methods: The genetic database of Hacettepe University, Department of Medical Biology, and clinical records of Hacettepe University Hospitals were analysed. Between January 1, 2000, and December 31, 2023, a total of 2640 patients harboring homozygous or compound heterozygous MEFV mutations were identified. Initial screening revealed 595 patients projected to be ≥50 years of age by 2024. Data were retrieved from the hospital electronic medical record system and complemented by structured telephone interviews in patients who could be contacted. Upon final evaluation, 281 patients with FMF aged ≥50 years with available clinical data were identified. Of these, 137 patients with documented attack frequency during the preceding 12 months were included in the analysis (Figure 1). Data collected included demographic characteristics, comorbidities, and family history; age at symptom onset and diagnosis; MEFV mutation profiles; attack characteristics at diagnosis and across the entire follow-up period; the presence of proteinuria and amyloidosis; and FMF-related therapies and corresponding dosages—including colchicine and anti–interleukin-1 inhibitors—administered at diagnosis and throughout follow-up. In addition, disease activity was assessed by recording the number of FMF attacks occurring within the preceding 12 months and the last 3 months.
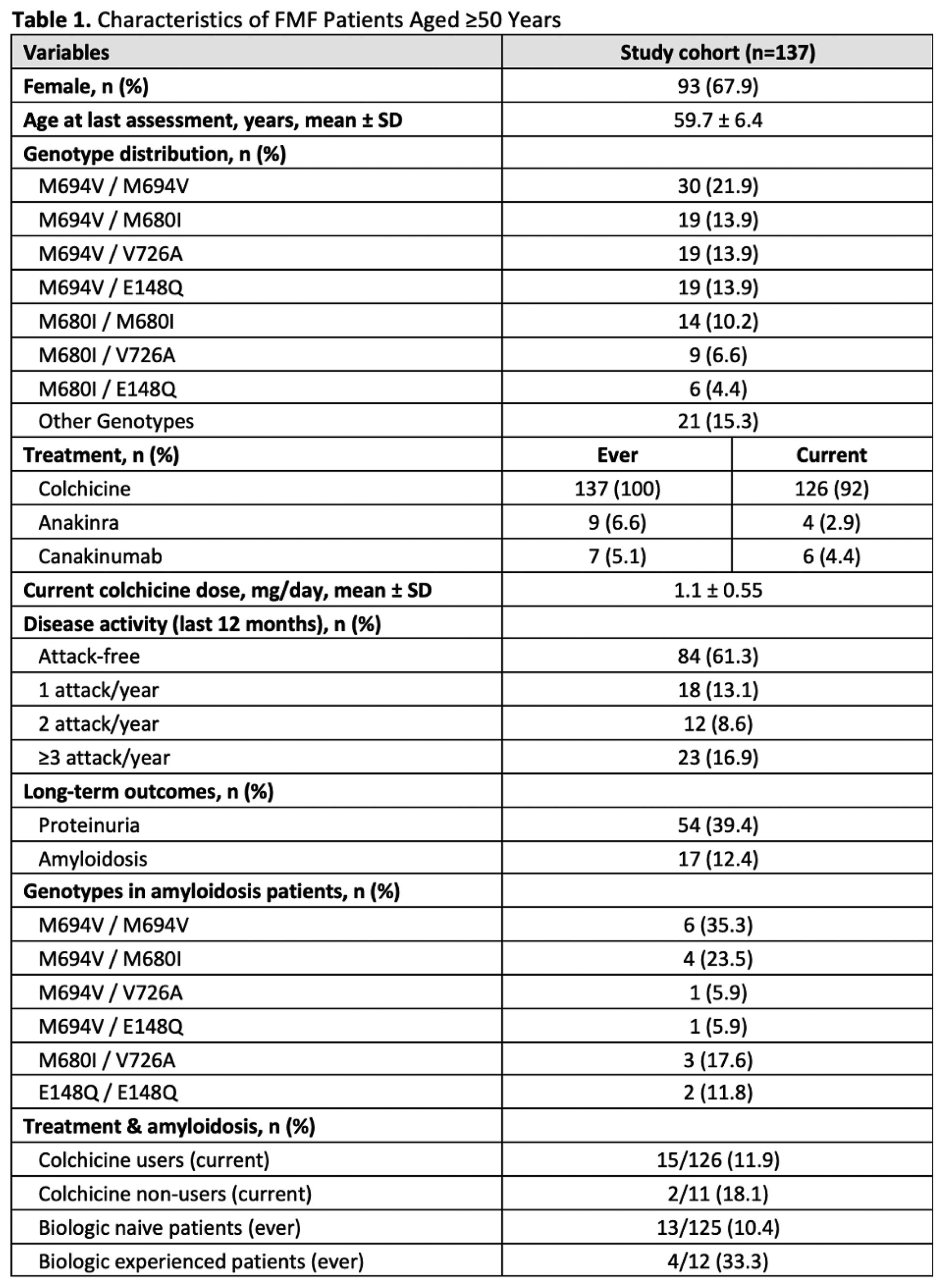
Results: The study included 137 patients (67.9% female) with a mean age of 59.7 ± 6.4 years at the last evaluation. The most frequent genotype was M694V homozygosity (21.9%), followed by M694V/M680I (13.9%), M694V/V726A (13.9%), and M694V/E148Q (13.9%). Regarding treatment, 92% of patients were currently on colchicine with a mean dose of 1.1 ± 0.55 mg/day. Biologic agents were used in a small group of patients; notably, retention appeared higher for canakinumab (6/7 current users) compared to anakinra (4/9 current users) (Table 1). Despite the advanced age of the cohort, disease activity persisted in a significant proportion of patients. Specifically, 38.7% of patients reported attacks within the last year, and a substantial subgroup (16.9%) suffering from a high disease burden characterized by frequent attacks (≥3 per year). An attack-free status during the preceding year was achieved in only 61.3% of the study population. Long-term damage was considerable; proteinuria was detected in 39.4% and amyloidosis in 12.4% of the patients. Amyloidosis was strongly linked to genotype, with 58.8% of affected patients carrying either M694V/M694V or M694V/M680I. In terms of treatment, the prevalence of amyloidosis was higher in patients who were not currently using colchicine (18.1%) compared to current users (11.9%). Furthermore, a higher prevalence was observed in biologic-experienced patients compared to biologic-naive ones (33.3% vs. 10.4%), reflecting the preferential use of anti-IL1 agents in patients with a more severe disease phenotype.
Conclusions: Our findings suggest that FMF does not uniformly attenuate with advancing age. Despite being over 50 years of age, a substantial proportion of patients continued to experience recurrent attacks and ongoing disease activity, challenging the concept of age-related disease quiescence. The continued need for biologic therapy in this population further highlights a subgroup with resistant disease. Moreover, the burden of long-term complications, particularly amyloidosis, underscores the importance of sustained disease control and lifelong colchicine prophylaxis. Therefore, rather than assuming age-related remission, clinicians should maintain careful vigilance for ongoing inflammation and organ damage through continued monitoring.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.