fetching data ... 
Background: Multigene autoinflammatory panels are increasingly used in adults with suspected autoinflammatory syndromes (AIS). In routine care, confirmatory yield is often limited and variants of uncertain significance (VUS) are frequent, making phenotype-driven test stewardship critical.
Objectives: To quantify real-world diagnostic yield and clinical utility of an autoinflammatory multigene panel in adults, and to assess whether targeted pre-test clinical suspicion is associated with higher final AIS diagnosis rates and post-test management changes.
Methods: Retrospective cohort study of all adults tested with an autoinflammatory multigene panel in a tertiary rheumatology service (2018–2025; n=171). Pre-test suspicion was classified as non-specific suspicion vs targeted suspicion (specific syndrome suspected: FMF/TRAPS/other AIS). Variants were analyzed in predefined core genes (MEFV, TNFRSF1A, NLRP3, MVK) and in additional panel genes, and classified as pathogenic/likely pathogenic (P/LP), VUS, or benign/likely benign. Final AIS diagnosis (confirmed/probable) was established by the treating team integrating phenotype and genetics. “Overall clinical yield” was defined as final AIS diagnosis and/or any P/LP variant. P/LP variants were considered genetically informative and not necessarily diagnostic per se. Clinical utility was defined as any post-test management change attributable to panel results, as recorded in clinical charts. Group comparisons used χ 2 /Fisher’s exact tests.
Results: The cohort was predominantly female (132/171, 77.2%); median age at testing was 42 years (IQR 33–53). Median diagnostic delay was 8 years (IQR 2–32; n=167). Most frequent manifestations were arthralgia without arthritis (127/171, 74.3%), recurrent fever (95/171, 55.6%), arthritis (90/171, 52.6%) and rash (64/171, 37.4%). Pre-test suspicion was non-specific in 162/171 (94.7%) and targeted in 9/171 (5.3%) (FMF 2/171, TRAPS 2/171, other AIS 5/171). No cases were referred with suspicion of CAPS or MKD, and no final CAPS/MKD diagnoses were made. Core-gene variants were found in 31/171 (18.1%): P/LP 6/171 (3.5%), VUS 23/171 (13.5%), benign/likely benign 2/171 (1.2%). Additional-gene variants were reported in 14/171 (8.2%): VUS/non-actionable 10/171 (5.8%), P/LP 2/171 (1.2%; IL36RN–DITRA and RNASEH2B), and benign/likely benign 2/171 (1.2%). P/LP variants in any gene were present in 8/171 (4.7%) (including 6 core-gene and 2 additional-gene P/LP). Final AIS diagnosis was established in 21/171 (12.3%) (confirmed 15/171, 8.8%; probable 6/171, 3.5%). Of these, 6/21 (28.6%) overlapped with P/LP variants (genetically supported), whereas 15/21 (71.4%) were clinical diagnoses without P/LP. In an exploratory analysis, abdominal pain was associated with final AIS diagnosis (10/21, 47.6% vs 25/150, 16.7%; Fisher p=0.0026), a hypothesis-generating finding that warrants validation. Targeted suspicion showed a numerically higher probability of final AIS diagnosis than non-specific suspicion (3/9, 33.3% vs 18/162, 11.1%), without reaching statistical significance (p=0.083). In the classic hereditary periodic fever subgroup (FMF/TRAPS suspicion; n=4), final AIS diagnosis was significantly more frequent (3/4, 75.0% vs 18/167, 10.8%; p=0.006). Overall clinical yield (final AIS diagnosis and/or any P/LP) was 23/171 (13.5%), with overlap between AIS diagnoses and P/LP findings. Clinical utility was observed: post-test management changed in 43/171 (25.1%), more often in patients with a final AIS diagnosis (14/21, 66.7%) than without (29/150, 19.3%). Management change occurred in 5/6 (83.3%) patients with core-gene P/LP variants and 10/23 (43.5%) with core-gene VUS, compared with 28/142 (19.7%) with non-informative core-gene results (negative/benign). Among patients receiving post-test targeted treatment (n=37), response was good/partial in 25/37 (67.6%).
Conclusions: In adult routine care, multigene autoinflammatory panels showed a modest diagnostic yield (21/171, 12.3%) with a substantial burden of non-definitive findings (core-gene VUS 23/171, 13.5%). Genetically informative P/LP variants were uncommon (8/171, 4.7%), yet panel results were associated with post-test management changes in one-quarter of patients (43/171, 25.1%). Diagnostic yield was higher when testing was focused on classic FMF/TRAPS phenotypes (3/4, 75.0% vs 18/167, 10.8%), whereas expanding beyond core genes mainly increased non-actionable additional-gene findings (10/171, 5.8%) and rarely identified actionable additional-gene P/LP variants (2/171, 1.2%). Among patients receiving post-test targeted treatment, a good/partial response was observed in 25/37 (67.6%). Overall, these findings support diagnostic stewardship in adults: phenotype-informed test selection, cautious interpretation of VUS, and limited incremental value of broad panel expansion in unselected patients.
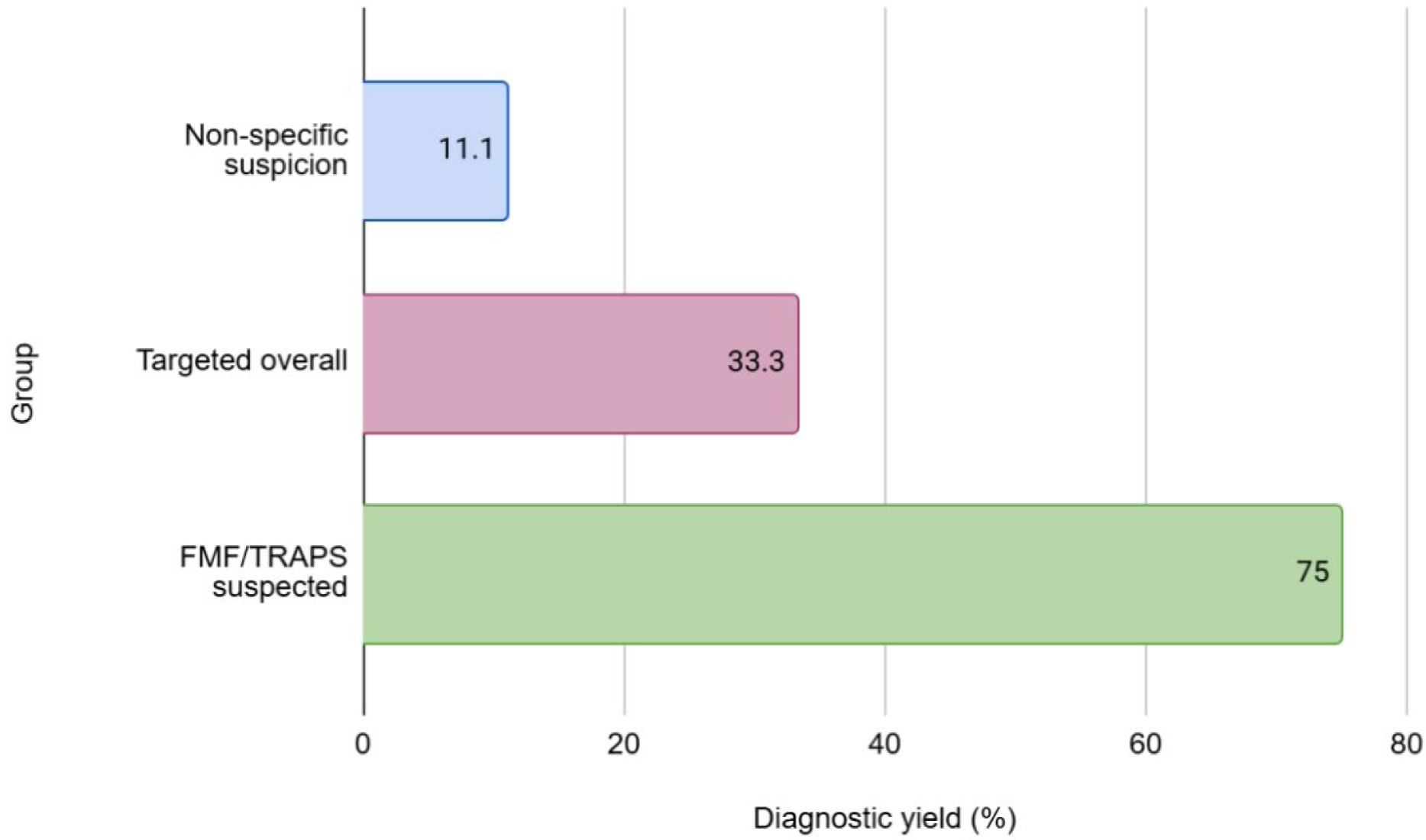
Diagnostic yield of the multigene panel by pre-test clinical suspicion. FMF/TRAPS suspicion had the highest AIS diagnosis rate (75.0%, 3/4) vs non-specific suspicion (11.1%, 18/162; p=0.006). Targeted overall showed a numerically higher yield than non-specific suspicion (33.3%, 3/9 vs 11.1%, 18/162), without reaching statistical significance (p=0.083).
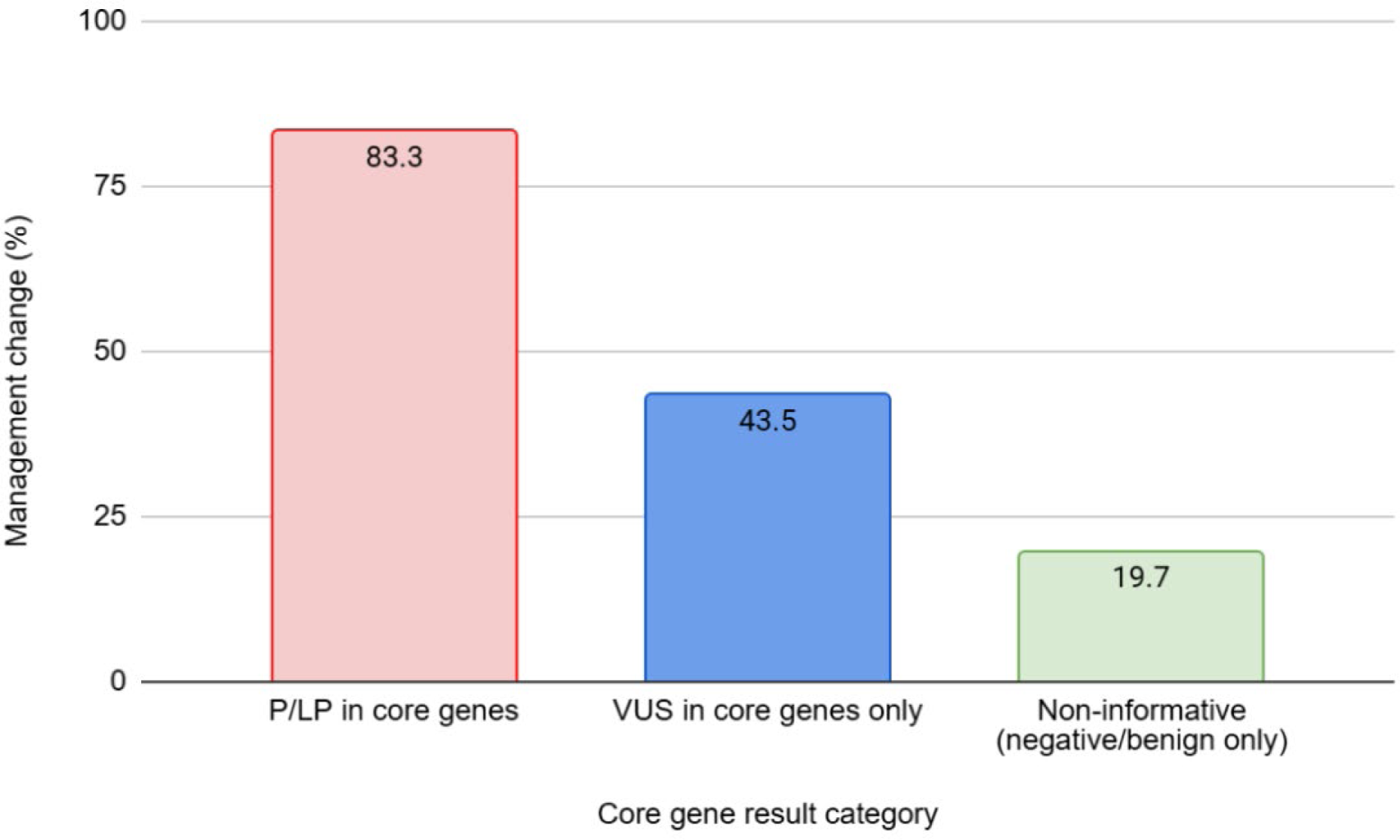
Post-test management change rates stratified by core gene test result category. Post-test management changes were highest with core-gene P/LP variants (83.3%), intermediate with core-gene VUS only (43.5%), and lowest with non-informative results (19.7%), showing a clear gradient across result categories.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.