fetching data ... 
Background: Sarcoidosis, a systemic inflammatory disease characterized by non-necrotizing granulomas and heterogeneous multiorgan involvement. Diagnosis is challenging due to the absence of a gold standard requiring compatible clinical and radiological findings, histological confirmation, and exclusion of alternative granulomatous diseases. In tuberculosis (TB)–endemic regions, differentiation from infectious granulomatous disorders is difficult, as mycobacterial antigens have been implicated as potential triggers. This is a case of systemic sarcoidosis following disseminated TB, highlighting this diagnostic overlap.
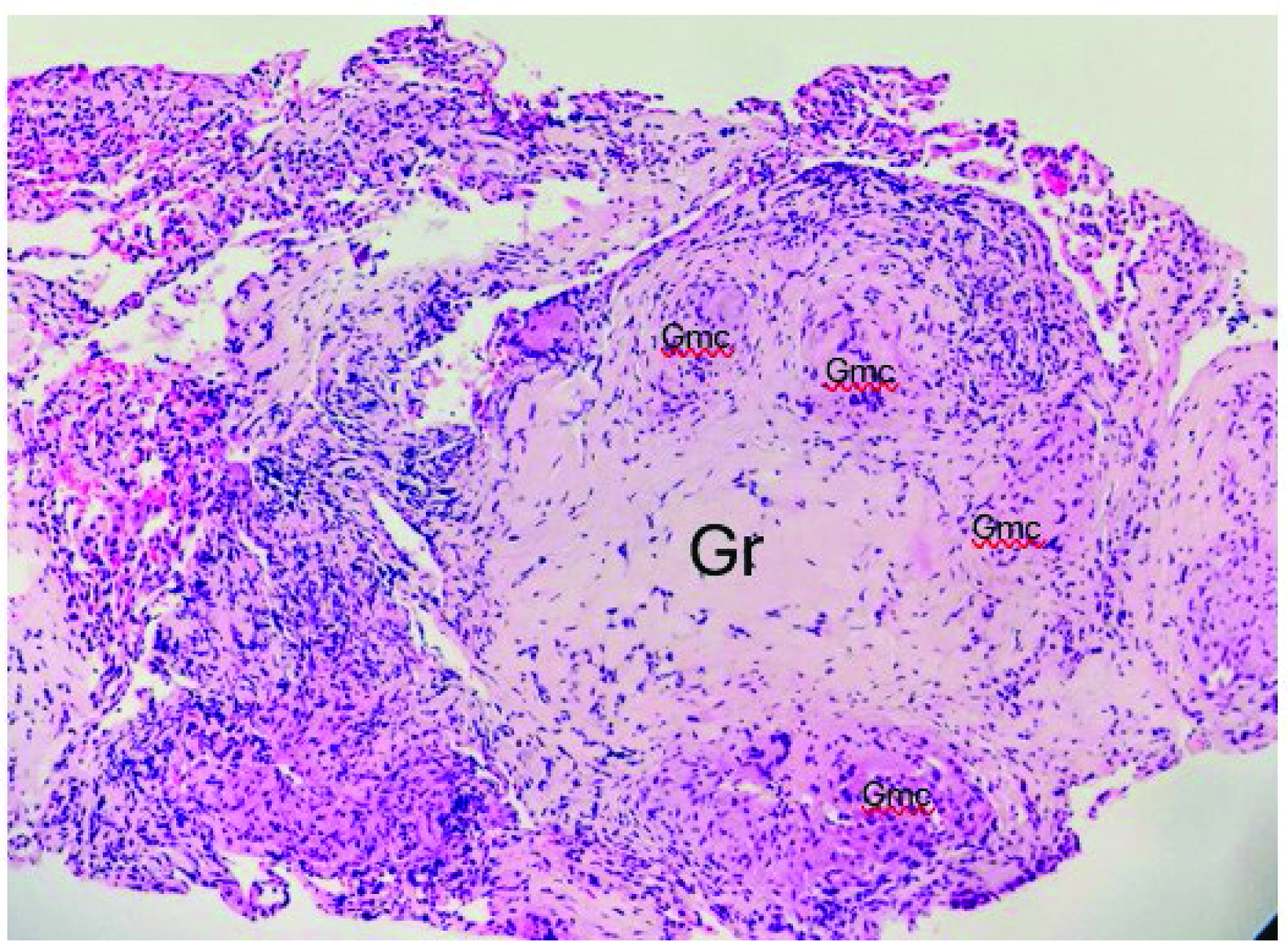
Case Presentation: A 37-year-old Black-man with HIV infection on stable antiretroviral therapy, diagnosed in 2023 with disseminated TB, confirmed by PCR and Ziehl–Neelsen staining. He required multiple surgical drainages and therapy modification due to rifampicin-induced hepatotoxicity. During TB treatment, he developed acute kidney injury with non-nephrotic proteinuria. Renal biopsy revealed granulomatous interstitial nephritis (GIN). Despite negative renal mycobacterial studies, renal involvement was attributed to TB. He completed 14 months of antituberculous therapy with clinical improvement. In 2025, he presented progressive visual loss, diplopia, dyschromatopsia, and dyspnea. Laboratory tests showed recurrent acute kidney injury and severe PTH-independent hypercalcemia. Brain MRI demonstrated bilateral optic nerve hyperintensity. Cerebrospinal fluid studies were unremarkable. Chest HRCT revealed new bilateral perilymphatic nodules and ground-glass opacities despite prior TB treatment. Bronchoalveolar lavage and microbiological studies were negative. Transbronchial biopsy showed non-caseating granulomas with negative infectious stains (figure 1). Other autoimmune diseases were excluded. Given recurrent GIN, hypercalcemia, neuro-ophthalmological involvement, and granulomatous lung disease without evidence of TB reactivation, a diagnosis of systemic sarcoidosis was established. He was treated with systemic steroids and cyclophosphamide. Clinical improvement after immunosuppression supported sarcoidosis without evidence of active tuberculosis.
Learning points for clinical practice: Previous tuberculosis confers a markedly increased risk of subsequent sarcoidosis, and recurrent granulomatous disease after adequate TB treatment should prompt reconsideration of sarcoidosis. Granulomatous interstitial nephritis is non-specific; PTH-independent hypercalcemia is a key discriminator favoring sarcoidosis over infection. Immune reconstitution in HIV may unmask sarcoidosis through a sarcoid-like inflammatory response. Neuro-ophthalmological involvement represents a severe, vision-threatening manifestation requiring prompt immunosuppression.
Transbronchial lung biopsy: Non caseating granuloma with extensive fibrosis. Gr: granuloma; Gmc: giant multinucleated cells.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.