fetching data ... 
Background: Responses to bDMARDs in RA vary widely, but we rarely have a practical way to read out what is happening in the synovium over time. Most blood biomarkers are either indirect or do not map cleanly onto synovial inflammatory programs. We therefore asked whether single-cell profiles from peripheral blood can capture synovium-relevant pathways and whether these signals change in step with treatment.
Objectives: To quantify how closely PBMC single-cell programs in RA align with synovial inflammatory pathways across independent synovial datasets, and test whether the shared blood–synovium programs are downregulated after CTLA-4–Ig therapy.
Methods: We performed scRNA-seq of PBMCs from untreated RA patients and healthy controls (HCs) to construct a peripheral immune atlas. Immune-state transitions were inferred using RNA velocity and pseudotime. For blood–synovium concordance, we identified upregulated pathways and differentially expressed genes (DEGs) in circulating monocytes and CD4 + T cells, and compared them with synovial transcriptomic signatures across eight independent public RA synovial datasets. Shared pathways were organised into pathway regulatory networks (PRNs) based on gene overlap and assessed by GSEA. Therapeutic modulation was evaluated by comparing pre- vs post-treatment PBMC profiles in RA patients receiving CTLA-4–Ig. Cell–cell communication changes were assessed using ligand–receptor interaction analysis.
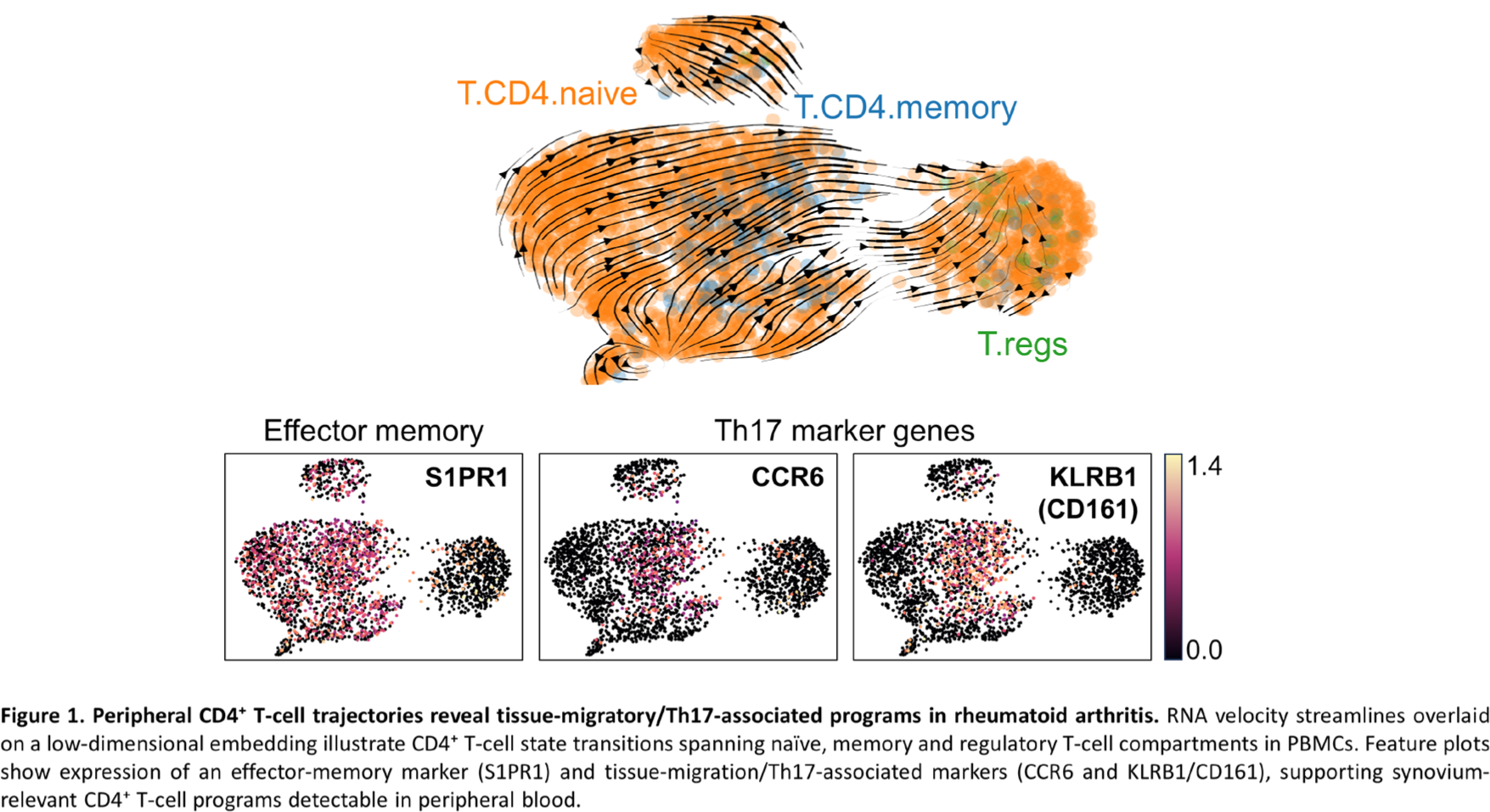
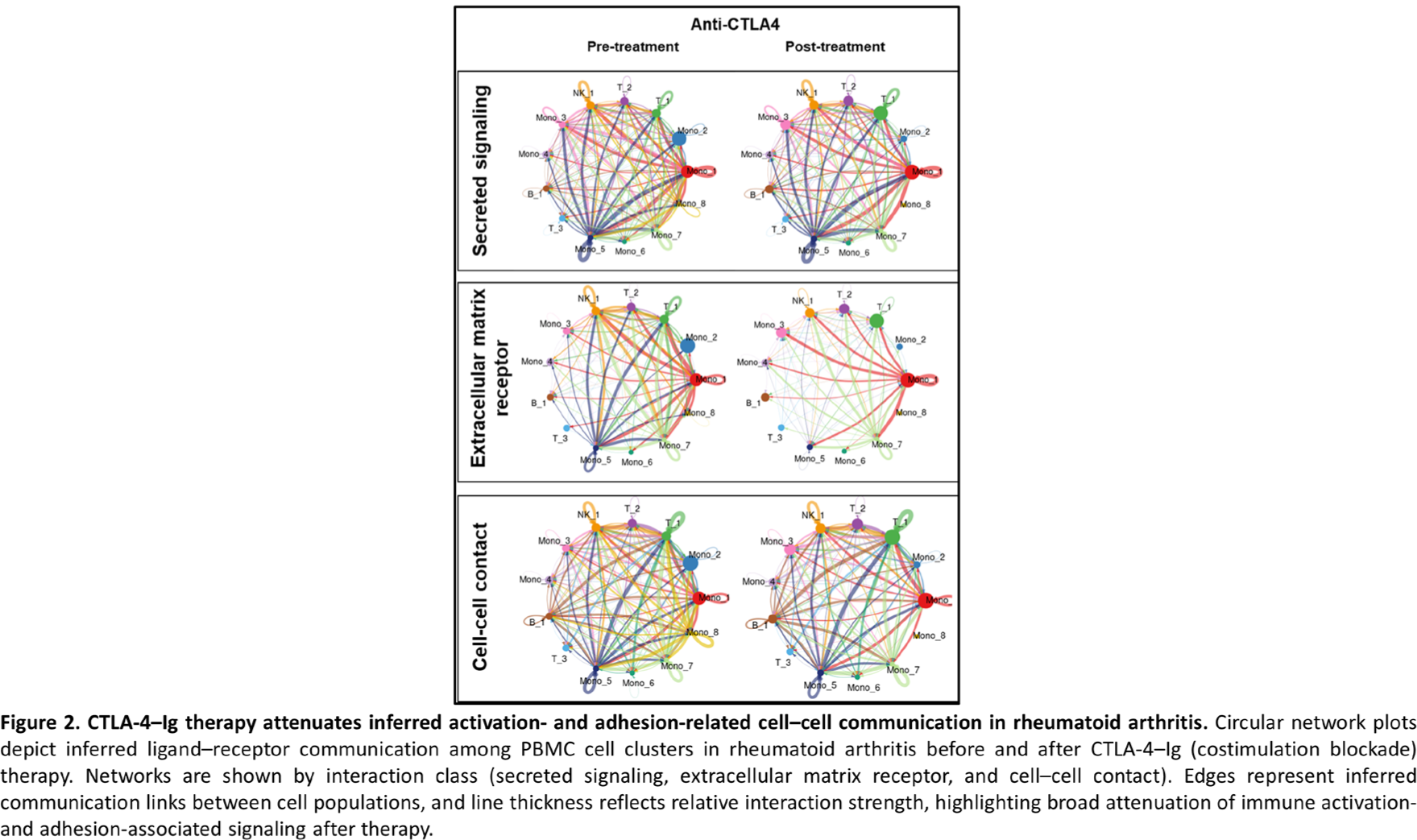
Results: A total of 60,253 high-quality PBMCs were resolved into 28 immune clusters. Trajectory analyses revealed RA-specific state transitions consistent with migratory and antigen-presenting programs that were absent in HCs (e.g., monocyte-to-DC differentiation with increasing CD1C, CSF2RA/CSF2RB and integrins; CD4 + trajectories with increasing CCR6/KLRB1 tissue-migration features) (Figure 1). Cross-tissue analysis demonstrated substantial concordance between blood and synovium: 1,386 of 3,230 upregulated pathways in RA blood monocytes overlapped with synovial pathway sets, and 725 of 1,572 upregulated pathways in RA blood CD4 + T cells overlapped with synovial pathways. Shared PRNs highlighted coherent modules related to lymphocyte activation, immune response, cell adhesion, and motility/migration. In monocytes, the shared blood–synovium pathways were strongly enriched for activation-related biology, including regulation of lymphocyte activation (NES 1.398, q=0.035), lymphocyte activation (NES 1.357, q=0.012) and regulation of cell activation (NES 1.452, q=0.005). We saw the same pattern in CD4 + T cells, where activation programs were also enriched (NES 1.303, q=0.042; NES 1.279, q=0.034). Following CTLA-4–Ig therapy, these blood–synovium shared inflammatory programs were significantly downregulated in both monocytes and CD4 + T cells (e.g., monocyte activation modules with negative enrichment: NES −1.444/−1.495/−1.450 with q-values <1×10 −4 ; CD4 + activation programs NES −1.318 and −1.377 with q≈0.03). Consistently, activation- and adhesion-related cell–cell communication was markedly attenuated post-therapy, supporting a systemic readout of therapeutic modulation (Figure 2).
Conclusions: Peripheral blood single-cell immune programs recapitulate key synovial inflammatory networks in RA and dynamically track CTLA-4–Ig–mediated modulation. Blood–synovium shared pathway modules provide a mechanistically anchored, non-invasive surrogate of synovial inflammation and therapeutic effects, supporting precision monitoring and biomarker development for bDMARD-treated RA.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.