fetching data ... 
Background: Social determinants of health (SDHs)—such as low income, unemployment, limited education, restricted access to healthcare, and racial/ethnic discrimination—contribute to health inequities and are associated with increased disease burden. In rheumatology, SDHs have been linked to worse clinical outcomes; for example, Latino patients experience delayed access to specialist care, higher disease severity at presentation, and poorer outcomes [1]. Analysis of these factors is challenging due to heterogeneous data collection and the sensitive nature of the information.
Objectives: To evaluate which social determinants of health (SDHs) are most frequently collected across cohorts within a collaborative network of immune-mediated inflammatory diseases, with the aim of developing a consensus on a minimum set of SDHs to be collected, along with recommendations for their implementation in cohorts.
Methods: The REI Network is a scientific collaboration comprising 31 multicentre academic research groups with individual registries collecting data on patients with immune-mediated inflammatory diseases across rheumatology, neurology, ophthalmology, and allergy. The network enables collaboration and secondary use of anonymised data to address research questions across disease areas. The PROGRESS framework is an acronym to identify characteristics that stratify health opportunities that may impact outcomes for a better interpretation of data in the context of potential inequity and was apply to identify SDHs [2]. Standardised information from 103 registries is stored in a common REDCap database, including detailed data dictionaries of all collected variables per cohort. We reviewed available data dictionaries to identify which SDHs were collected across cohorts.
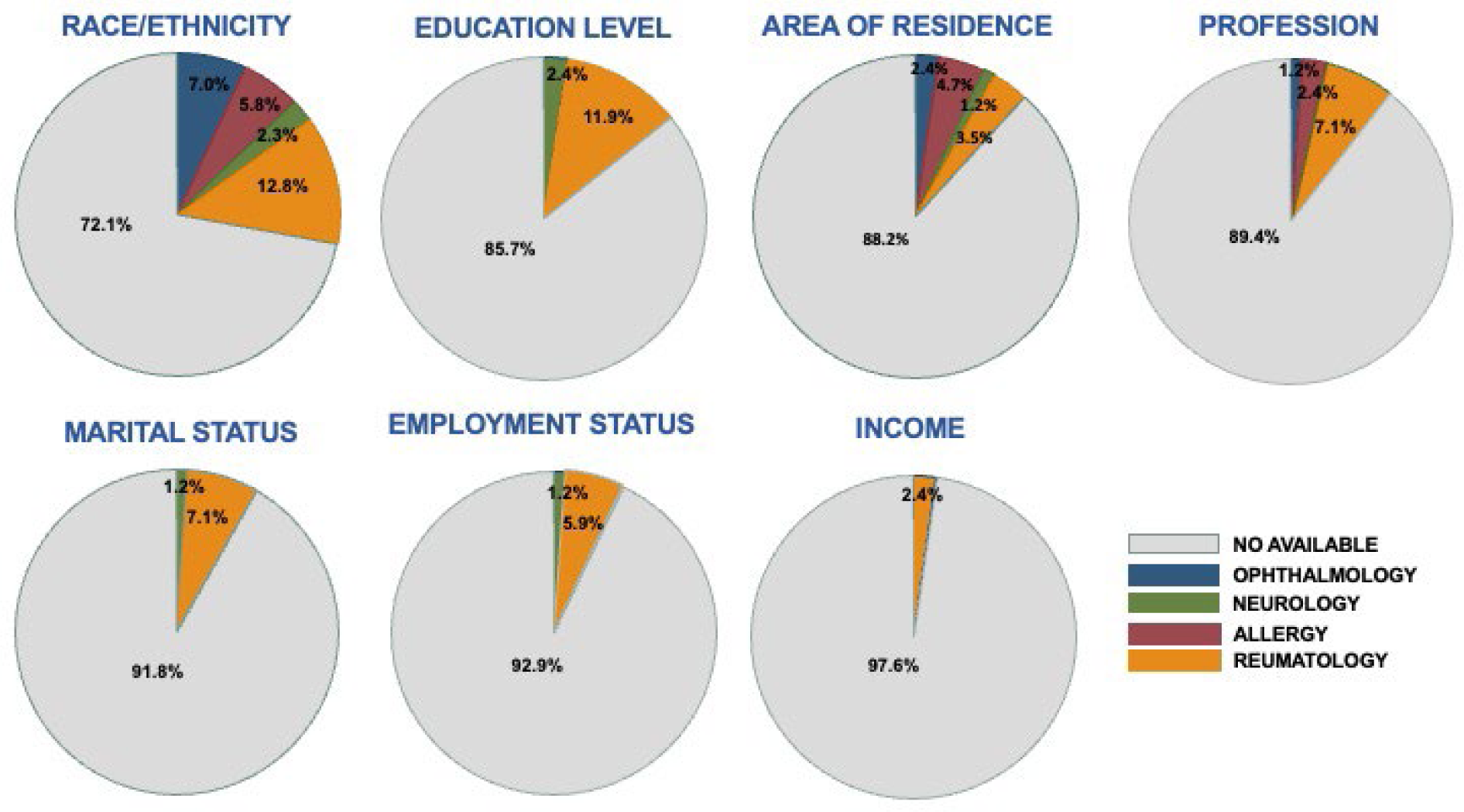
Results: A total of 103 cohorts were reviewed, of which 86 had an available data dictionary. These included 23 (29.5%) rheumatology cohorts including patients with the following diagnosis: rheumatoid arthritis, spondyloarthritis, lupus, and osteoarthritis; 34 (31.9%) ophthalmology cohorts including patients with macular degeneration and uveitis; 15 (16.2%) neurological cohorts including patients with multiple sclerosis and Parkinson’s disease; and 15 (16.2%) allergy cohorts including patients with drug and food allergies and anaphylaxis. Overall, rheumatology cohorts most frequently collected SDHs, with the exception of area of residence, which was more frequently collected in allergy cohorts (Figure). The most commonly recorded SDH was race/ethnicity, reported in 2.3–12.5% of registries of the four specialities. Educational level was only collected in neurology (2.4%) and rheumatology cohorts (11.9%). Area of residence (urban/rural) (1.2-4.7%), and profession (1.2-7.1%) were less frequently collected. Marital status and employment status were only collected in rheumatology and neurology cohorts, and income only in 2.4% of rheumatology cohorts.
Conclusions: Overall, SDHs are infrequently collected across registries. When recorded, they most commonly include race/ethnicity, educational level, area of residence, and profession, while marital status, employment status, place of birth, and income are rarely captured. These findings underscore the need to develop a consensus on a minimum set of SDHs that should be systematically collected in cohorts, as well as recommendations for their standardised implementation.
Most commonly collected SDH in the different cohorts by speciality
REFERENCES: [1] Riad M, et al. Journal of clinical rheumatology 2020, 26(7):279-284).
[2] PROGRESS-Plus. Cochrane Equity [Internet]. Available:
Acknowledgments: NIL.
Disclosure of Interests: Ana Triguero-Martinez: None declared, Lucia Comino-Maroto: None declared, Juan Molina-Collada: None declared, Miren Uriarte-Ecenarro: None declared, Sara Llorente-González: None declared, Ainara Chas: None declared, Isidoro González-Álvaro: None declared, Isabel Castrejon AbbVie, AstraZeneca, Boehringer, GSK, Lilly, Pfizer,, Advanz Pharma, Alfasigma, UCB.