fetching data ... 
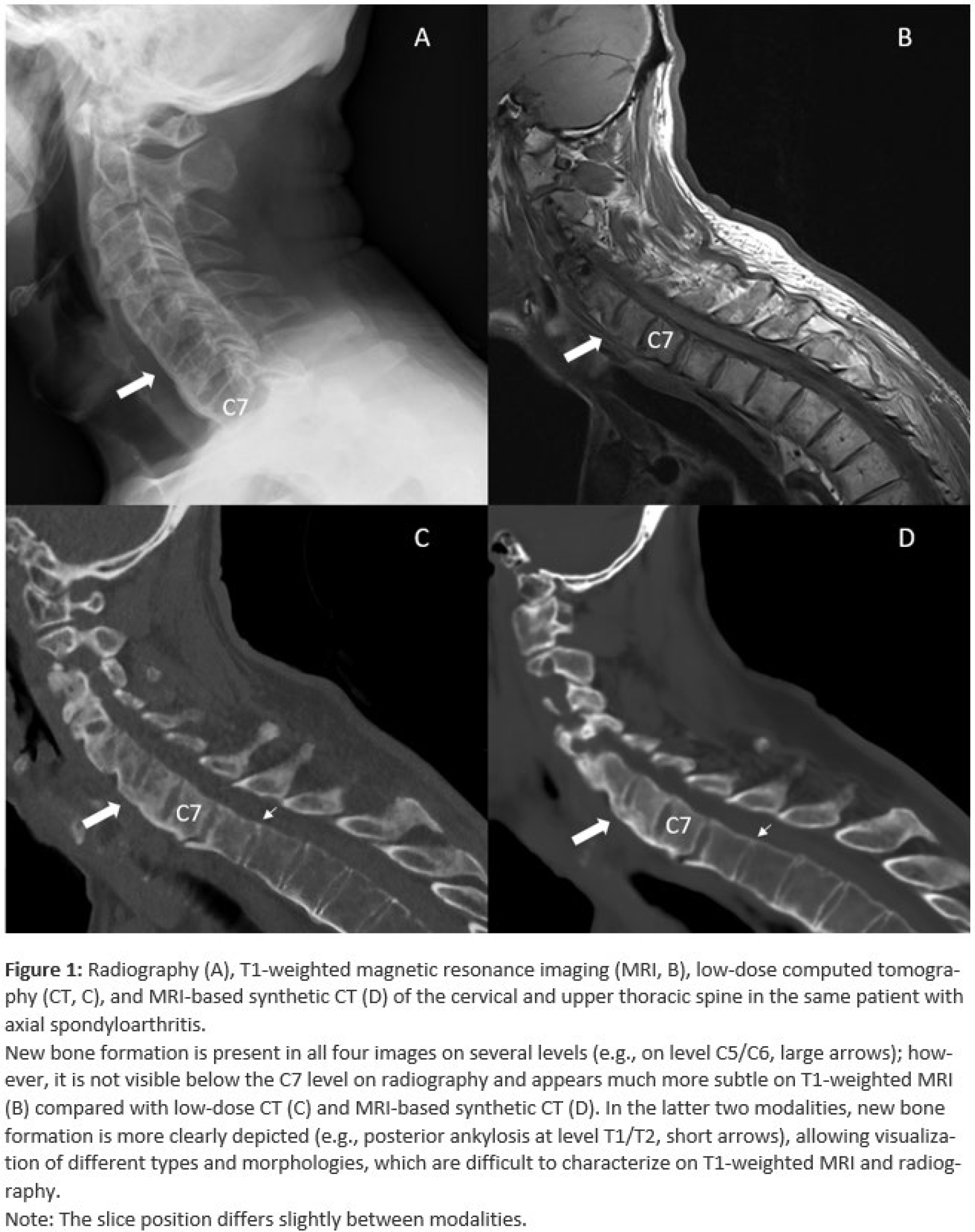
Background: Preventing functional decline by limiting spinal structural damage, especially new bone formation (NBF), is a central treatment goal in axial spondyloarthritis (axSpA); however, evaluating whether therapies can halt this process is restricted by current imaging modalities. Radiography scored with the modified Stokes Ankylosing Spondylitis Spinal Score (mSASSS) remains the ASAS/OMERACT-recommended method. Nevertheless, radiography’s low sensitivity to change means that long follow-up periods, typically two years, are required. Consequently, it is not suitable for assessing structure-modifying effects in randomized clinical trials. Magnetic resonance imaging (MRI) is sensitive to detect inflammation, though it provides less information about spinal NBF (Figure 1). Computed tomography (CT) is the gold standard for visualizing bone, but it is not routinely used in clinical practice or trials due to the high dose of radiation it involves. These challenges underline the need for alternative imaging techniques to assess spinal structural damage. MRI-based synthetic CT (sCT) produces CT-like images without the use of ionizing radiation, enabling detailed visualization of spinal bone structures. In a previous pilot study of 17 patients with axSpA [1], we found that sCT detected spinal NBF more effectively than radiography when compared with low-dose CT. However, this study was limited by its small sample size, inclusion of only patients with a single diagnosis, and absence of a healthy control group. In addition, comparisons were made only with low-dose CT and radiography, and not with T1-weighted MRI. Here, we therefore intend to build on these findings and further evaluate the potential of sCT as a radiation-free spinal imaging method.
Objectives: This study aims to compare the performance of sCT, T1-weighted MRI, low-dose CT, and radiography in detecting spinal NBF in patients with inflammatory arthritides and healthy controls (HC).
Methods: Patients with a diagnosis of either axSpA according to the ASAS classification criteria, psoriatic arthritis (PsA) according to the CASPAR criteria, or rheumatoid arthritis (RA) according to the ACR/EULAR 2010 criteria, were recruited between July 2023 and August 2024. HCs were recruited through a poster in the same period. All participants underwent low-dose CT and MRI of the entire spine. Additionally, patients (not HCs) received cervical and lumbar spine radiography according to the mSASSS recommendations. sCT was reconstructed using the BoneMRI application v1.8. All images were pseudonymized and independently assessed for the presence of new bone formation by two experienced readers blinded to all other imaging and clinical information, including diagnosis. One reader repeated the assessment of low-dose CT and sCT images 6 months after the initial read. Descriptive statistics were performed, and the sensitivity and specificity of sCT, T1-weighted MRI, and radiography were calculated using low-dose CT as the reference standard. Inter-reader and intra-reader reliability were assessed using a two-way random effects single measure model of intraclass correlation coefficient (ICC) based on absolute agreement for sum scores on patient level.
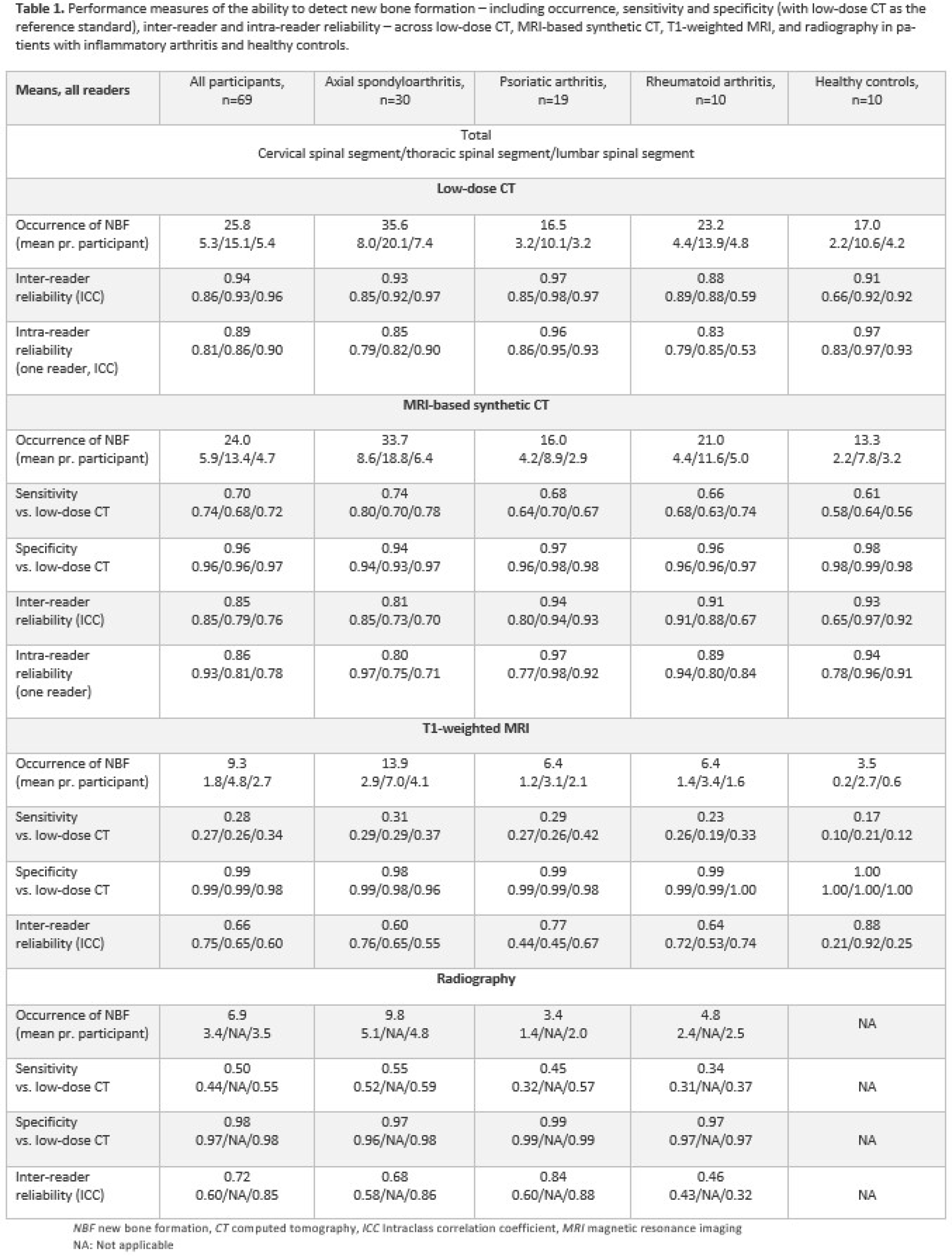
Results: A total of 69 participants were included (33 females, mean age 51.4 years): 30 with axSpA, 19 with PsA, 10 with RA, and 10 HCs. Among all participants, the mean number of NBFs scored per participant was 25.8 on low-dose CT, 24.0 on sCT, 9.3 on T1-weighted MRI, and 6.9 on radiography (Table 1). The axSpA group consistently demonstrated the highest mean number of NBFs per participant across all modalities (35.6 on low-dose CT, 33.7 on sCT, 13.9 on T1-weighted MRI, and 9.8 on radiography). Using low-dose CT as the reference standard, the overall sensitivity for detecting NBFs was 0.70 for sCT, 0.28 for T1-weighted MRI, and 0.50 for radiography (Table 1). Specificity was ≥0.94 for all three imaging methods. The overall inter-reader reliability (Table 1) was excellent for both low-dose CT and sCT, and fair to good for radiography and T1-weighted MRI. Intra-reader reliability for detecting NBFs across all participants was 0.89 for low-dose CT and 0.86 for sCT.
Conclusions: This study presents the first comprehensive comparison of MRI-based synthetic CT, T1-weighted MRI, low-dose CT, and radiography in detecting new bone formation in the spine. By evaluating a cohort of patients with axSpA, PsA, and RA in addition to healthy controls, we thoroughly examined and compared the performance of each imaging technique in detecting NBF throughout the entire spine. Using low-dose CT as the reference standard, sCT demonstrated markedly higher sensitivity than both T1-weighted MRI and radiography. Inter-reader and intra-reader reliability were comparable between low-dose CT and sCT, suggesting that discrepancies in lesion detection are more likely due to reader variability than to missed lesions by sCT itself. These findings highlight the potential of sCT as a future method for evaluating spinal structural damage in clinical practice and trials.
REFERENCES: [1] Willesen ST, Hadsbjerg AE, Møller JM, et al. MRI-based synthetic CT: a new method for structural damage assessment in the spine in patients with axial spondyloarthritis - a comparison with low-dose CT and radiography. Ann Rheum Dis. 2024;83:807-15.
Acknowledgments: NIL.
Disclosure of Interests: Simone Tromborg Willesen: None declared, Jakob Møllenbach Møller: None declared, Kasper K Gosvig: None declared, Susanne Juhl Pedersen AbbVie, Novartis and UCB, Anna E F Hadsbjerg Novartis and UCB, Stylianos Georgiadis Novartis, AbbVie and UCB, Mikkel Østergaard Abbvie, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, Gilead, Hospira, Janssen, MEDAC, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi, UCB, Abbvie, BMS, Boehringer Ingelheim, Celgene, Eli Lilly, Galapagos, Gilead, Hospira, Janssen, MEDAC, Merck, Novartis, Novo, Orion, Pfizer, Regeneron, Roche, Sandoz, Sanofi, UCB, AbbVie, Amgen, BMS, Merck, Celgene, Eli Lilly, Novartis, UCB.