fetching data ... 
Background: Fibromyalgia (FM) diagnosis remains challenging due to subjective symptom presentation, absence of objective biomarkers, and significant clinical overlap with inflammatory rheumatic and musculoskeletal diseases (RMDs). The average diagnostic delay of 5-7 years from symptom onset contributes to patient suffering and healthcare burden. Recent advances in artificial intelligence have enabled novel diagnostic approaches. Large language model (LLM)-driven sentiment analysis of patient transcripts can distinguish FM from chronic pain conditions with 87% accuracy and 84% sensitivity [1]. However, text-only analysis may miss critical non-verbal pain and emotional distress markers that are clinically observable in FM patients. We developed fAI-BRO (Fibromyalgia AI-Based Rheumatology Observer), a multimodal approach integrating AI-powered facial expression analysis with psycholinguistic transcript evaluation to capture both verbal and non-verbal FM indicators, hypothesizing that this would improve diagnostic performance.
Objectives: To evaluate the diagnostic accuracy, specificity, and patient acceptability of fAI-BRO multimodal sentiment analysis in distinguishing FM from inflammatory arthritis and other rheumatic diseases, and to compare performance with the previous text-only sentiment analysis approach.
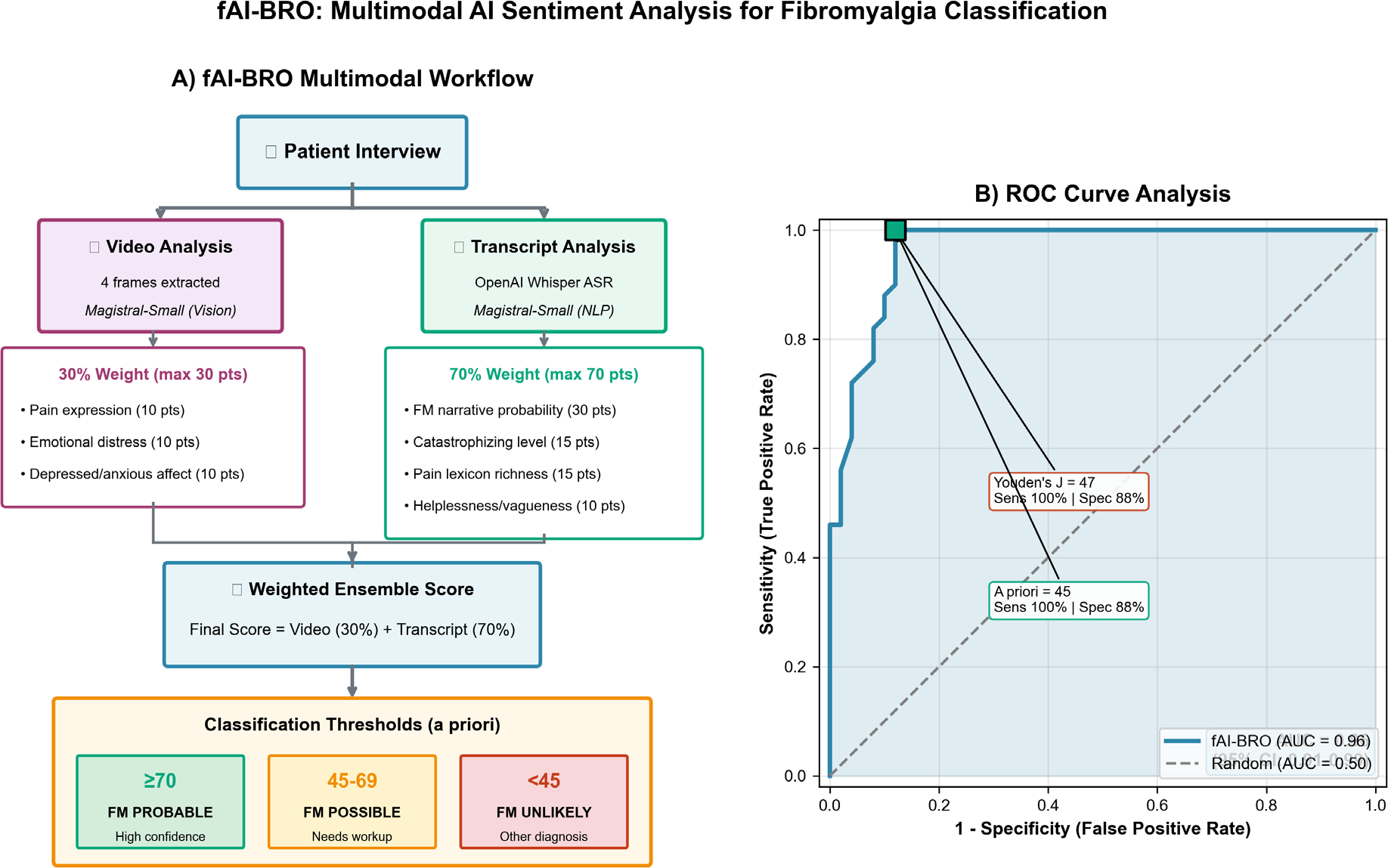
Methods: Cross-sectional proof-of-concept study conducted at University of Bari Rheumatology Unit. FM patients meeting ACR 2016 criteria (n=50) were compared with RMD patients (n=50) including: rheumatoid arthritis (RA, n=12), psoriatic arthritis (PsA, n=13), spondyloarthritis (SpA, n=8), systemic lupus erythematosus (SLE, n=3), dermatomyositis (n=3), polymyalgia rheumatica (PMR, n=3), knee osteoarthritis (OA, n=5), and subacromial impingement (n=3). fAI-BRO employed zero-shot multimodal sentiment analysis using Magistral-Small (Mistral AI) deployed locally via LM Studio without fine-tuning on FM-specific training data, ensuring generalizability. The weighted ensemble scoring algorithm generated scores from 0-100 points integrating two components with a priori weights established based on prior evidence (1): **Video analysis component (30% weight, max 30 points):** Four evenly-distributed frames were extracted from patient interviews and analyzed for: (a) pain expression indicators including facial grimacing and tension (10 points); (b) emotional distress level based on average emotional state score (10 points); and (c) depressed or anxious affective states detected across frames (10 points). **Transcript analysis component (70% weight, max 70 points):** OpenAI Whisper performed automatic speech recognition. Psycholinguistic analysis assessed: (a) FM narrative probability reflecting overall linguistic profile match (30 points); (b) catastrophizing level including magnification, rumination, and helplessness language (15 points); (c) affective and sensory pain lexicon richness (15 points); and (d) helplessness and cognitive dysfunction (vagueness) markers (10 points). All evaluated parameters were defined by expert rheumatologist consensus based on validated FM constructs including the Pain Catastrophizing Scale and McGill Pain Questionnaire dimensions. Classification thresholds were established a priori following clinical probability conventions: <45 = FM Unlikely, 45-69 = FM Possible, ≥70 = FM Probable. For diagnostic performance calculations, scores ≥45 (Possible + Probable) were classified as FM-positive. ROC curve analysis with Youden’s J index validated threshold selection. Patient acceptability was assessed via 5-point Likert scale for comfort and binary validation of facial sentiment agreement.
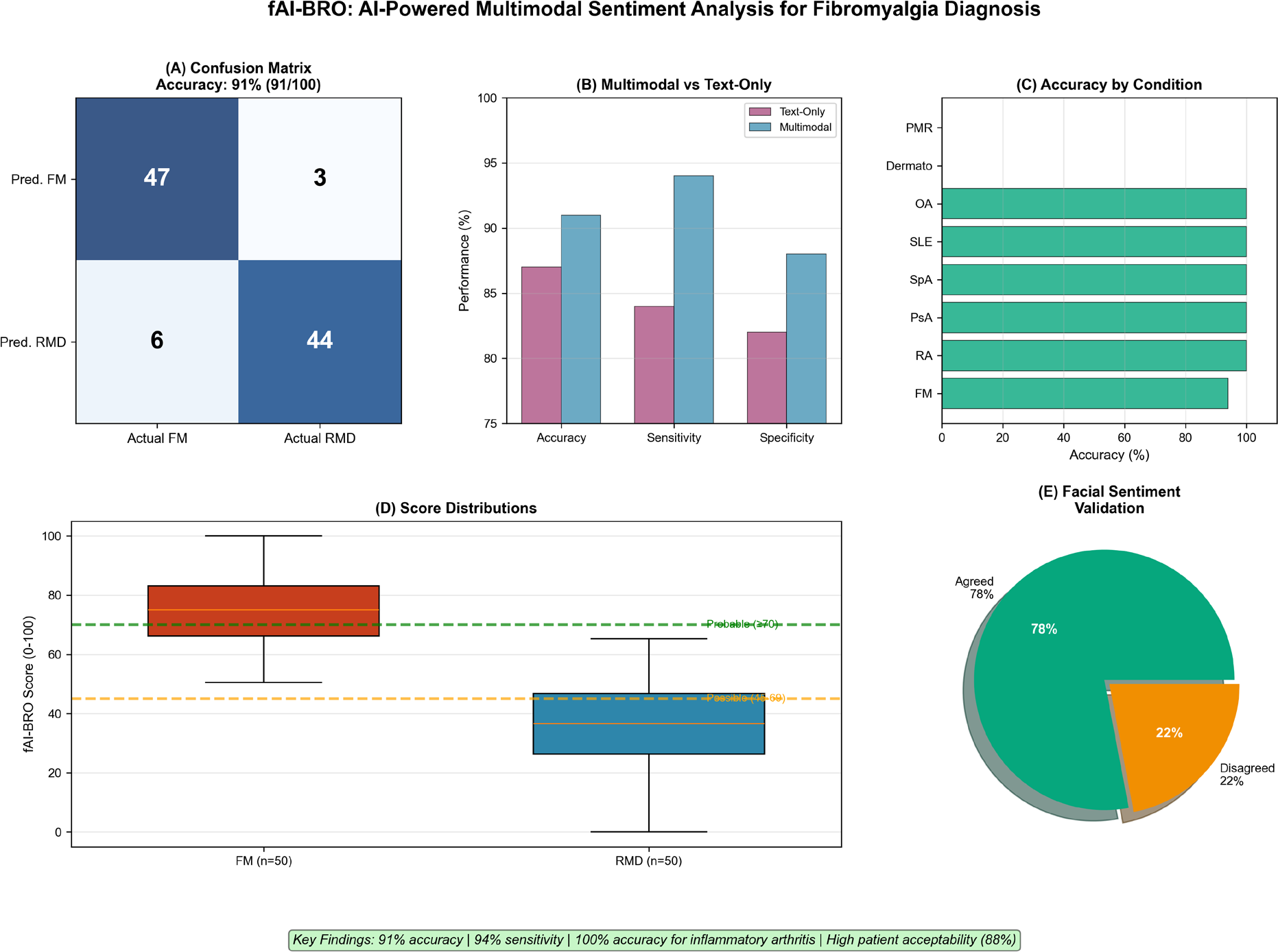
Results: Patient demographics showed FM patients were younger (46±8 vs 53±14 years, p<0.01) and predominantly female (84% vs 54%, p<0.001), consistent with FM epidemiology. fAI-BRO achieved 91% overall accuracy (95% CI: 83.6-95.8%), 94% sensitivity (95% CI: 83.5-98.7%), 88% specificity (95% CI: 75.7-95.5%), 88.7% positive predictive value, and 93.6% negative predictive value. ROC analysis demonstrated excellent discrimination with AUC 0.96 (95% CI: 0.91-0.99). Youden’s J index identified 47 as the optimal classification threshold, providing statistical validation for the a priori 45-point cut-off. Subgroup analysis revealed perfect classification (100% accuracy) for all inflammatory arthritis subtypes (RA, PsA, SpA, SLE; n=36) and mechanical conditions (OA, subacromial impingement; n=8). All six false positives (12%) occurred exclusively with dermatomyositis (n=3; mean score 57±11) and PMR (n=3; mean score 66±3), both scoring in the ‘FM Possible’ range (45-69). Three FM patients (6%) were false negatives. Score distributions differed significantly between groups: FM patients scored 69±10 vs other RMD 32±7 (p<0.001). Notably, while inflammatory arthritis and mechanical conditions uniformly scored <45, PMR and dermatomyositis exhibited scores overlapping with the FM distribution, possibly reflecting shared phenotypic features (widespread muscle pain, fatigue, emotional distress). Mean processing time was 324±45 seconds (5.4 minutes), clinically feasible for routine use. Patient acceptability was high: 88% rated comfort ≥4/5 (mean 4.5±0.7) and 78% agreed with the facial sentiment detection. Compared to the text-only sentiment analysis approach, the multimodal approach achieved +4% accuracy improvement (91% vs 87%) and +10% sensitivity improvement (94% vs 84%), demonstrating the added diagnostic value of facial expression analysis.
Conclusions: fAI-BRO multimodal sentiment analysis achieved 91% accuracy and 94% sensitivity for FM classification, with perfect discrimination of inflammatory arthritis. PMR and dermatomyositis misclassification reflects shared phenotypic features, appropriately triggering ‘Possible’ classification requiring biomarker workup. A user-friendly GUI has been developed for clinical use (demo video: zttps://drive.google.com/file/d/1tAu1FWRoCUwBIgQDvQ6D9aUNejTaq7Bo/view). Multi-center validation is warranted.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.