fetching data ... 
Background: Insomnia, depression, and fatigue are common symptoms in patients with rheumatoid arthritis (RA), which significantly impact their quality of life (QOL)[1]. These deteriorations in QOL are also known to correlate with worsening disease activity in RA. One of the most commonly used patient-reported outcome measures for QOL is the EuroQol-5 Dimensions (EQ-5D), which provides subjective QOL assessment across five dimensions: mobility, self-care, daily activities, pain/discomfort, and anxiety/depression; however, it is subject to recall bias and may not be optimal for conducting real-time longitudinal assessments. In contrast, wearable devices provide continuous objective data, such as physical activity, sleep patterns, and heart rate variability (HRV). While we have previously reported their association with RA disease activity [2], these metrics may further serve as potential biomarkers for QOL.
Objectives: This study aims to evaluate the association between EQ-5D scores and wearable device-derived data in patients with RA. By leveraging machine learning, we seek to identify wearable metrics that can objectively assess subjective QOL, ultimately aiming to enhance precision medicine approaches.
Methods: In this prospective observational study, patients with RA were enrolled and provided with wrist-worn smartwatches (Fitbit Sense2, Google LLC, CA, USA) for continuous monitoring. EQ-5D-5L questionnaire assessments were compared with indicators from wearable devices during the preceding 7-day period prior to EQ-5D questionnaire completion. Days with <80% device wear time were excluded from analysis. The associations between the EQ-5D utility score and wearable-derived data were evaluated using Pearson and partial correlation coefficients, adjusted for potential covariates. Binary classification models were developed using wearable-derived data to predict high-scoring (EQ-5D > median) and low-scoring (EQ-5D ≦ median) groups. For this analysis, the EQ-5D utility score was dichotomized at the median to serve as the target variable. In an extreme groups analysis, binary classification models were implemented to predict poor (lowest quartile) versus high (highest quartile) EQ-5D scores, excluding participants in the interquartile range. Five-fold cross-validation was performed. To identify the most influential wearable-derived features and enhance model interpretability, SHapley Additive exPlanations (SHAP) analysis was employed. This approach quantifies the contribution of each feature to individual predictions.
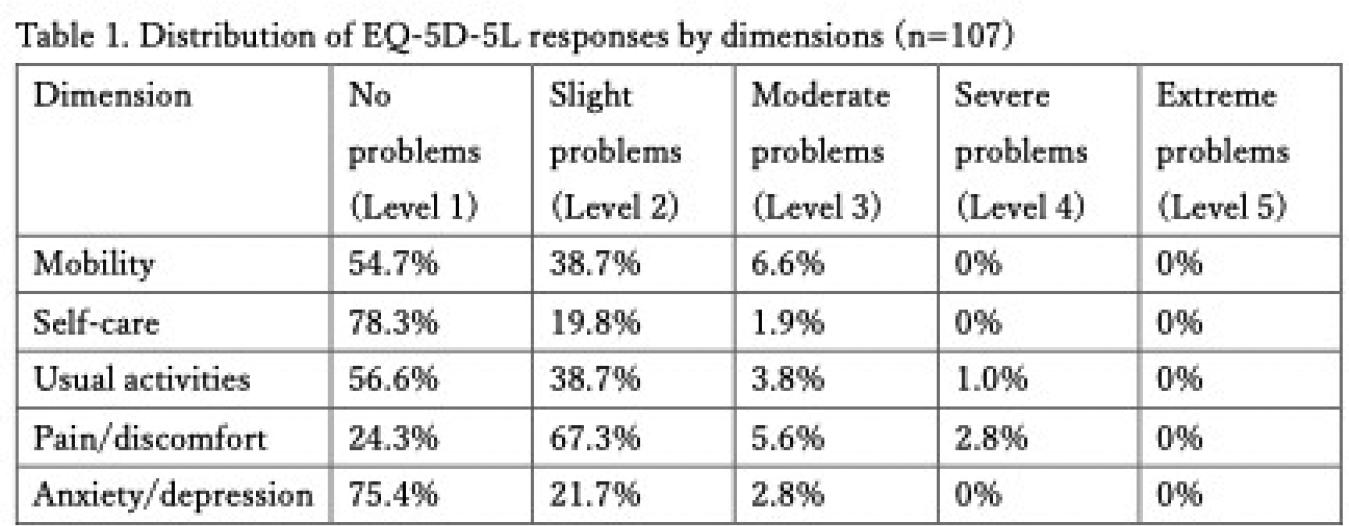
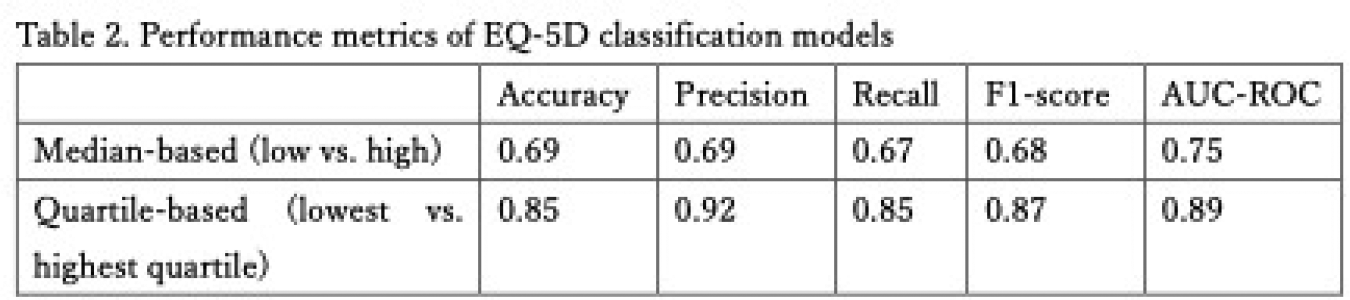
Results: A total of 129 patients were enrolled, of whom 107 patients with RA provided complete the questionnaires and were included in the final analysis. The median age was 55 years (IQR 46–66), 84% were female, and the median disease duration was 82 months (IQR 5–162). Glucocorticoids were used in 15.9% of patients, methotrexate in 77.6%, tumor necrosis factor inhibitors in 20.1%, interleukin-6 receptor inhibitors in 29.0%, and Janus kinase inhibitors in 9.3% of patients. The median disease activity score (DAS) 28-CRP was 2.5 [1.7-2.9], clinical disease activity index (CDAI) was 6.6 [2.3-10.7], simplified disease activity index (SDAI) was 6.6 [2.3-11.0], and health assessment questionnaire-disability index was 0.8 [0.4-1.0]. EQ-5D utility score was 0.83[0.74–0.90]. The distribution of patient-reported responses for each EQ-5D-5L dimension is shown in Table 1. The EQ-5D utility scores correlated with daytime HRV parameters ( r = 0.59, p <0.05), sleep HRV parameters ( r = -0.53, p <0.05), and daily metabolic equivalents × hours during sleep ( r =0.29, p <0.05). Among the EQ-5D dimensions, mobility (Dimension1), self-care (Dimension2), usual activities (Dimension3), and pain/discomfort (Dimension4) demonstrated significant correlations with daytime HRV parameters ( r =0.51, 0.46, 0.46, and 0.46, respectively; all p <0.05), while anxiety/depression (Dimension5) correlated with heart rate recovery (percentiles) ( r =0.50, p <0.05). The EQ-5D utility score was significantly correlated with disease activity scores, including DAS28-CRP ( r =−0.45), CDAI ( r =−0.43), and SDAI ( r =−0.43)(respectively; all p <0.05). Performance metrics for the classification models are summarized in Table 2. Both the median-based (low vs. high) and quartile-based (lowest vs. highest quartile) EQ-5D models demonstrated strong discriminative capacity, yielding AUC-ROC values of 0.75 and 0.89, respectively. SHAP analysis identified daytime HRV metrics and sleep duration as top predictors for EQ-5D classification models. In the full dataset analysis, the weekly median and standard deviation (SD) of daytime HRV, along with sleep duration, accounted for ≥10% of the total feature importance. In the quartile-based analysis, the weekly mean and SD of daytime HRV consistently showed high contributions of ≥10%.
Conclusions: In patients with RA, wearable-derived physiological and behavioral data showed moderate correlations with EQ-5D utility scores that were comparable to conventional disease activity indices. Furthermore, the machine learning–based binary classification model demonstrated high discriminatory power for EQ-5D utility states using wearable-derived parameters. SHAP analysis identified daytime HRV metrics and sleep duration as the top predictors, each contributing ≥10%. These findings suggest that wearable data integrated with machine learning can objectively reflect patient-reported QOL and serve as a real-time digital biomarker in clinical practice.
(M HK and KI are contributed equally.)
REFERENCES: [1] Higashida-Konishi M, Izumi K, et al . Association of disease activity with insomnia, depression, and fatigue in patients with rheumatoid arthritis: a multicenter prospective observational study. ACR. 2025. November 24-29. Chicago, United States.
[2] Izumi K, Higashida-Konishi M, et al . Digital biomarker for disease activity in rheumatoid arthritis using wrist-worn wearable device-acquired sensing data: a multicenter single-arm prospective study (interim report). Ann Rheum Dis 2024;83:1587-1588.
Acknowledgments: NIL.
Disclosure of Interests: Misako Higashida-Konishi: None declared, Keisuke Izumi Asahi Kasei, Chugai, Abbvie, Eisai, Gilead Sciences, and Teijin Pharma, Shuntaro Saito: None declared, Hiroki Tabata: None declared, Satoshi Hama: None declared, Tatsuhiro Oshige: None declared, Yutaka Okano: None declared, Hisaji Oshima: None declared, Katsuya Suzuki AbbVie, Asahi Kasei, Boehringer Ingelheim, Chugai, Eisai, Eli Lilly, Gilead, GlaxoSmithKline, Mitsubishi Tanabe, Pfizer, Sanofi, Taisho, UCB, and Viatris, Yasumasa Mashimo: None declared, Jiro Sakamoto: None declared, Toshikazu Fukami: None declared, Kazumichi Minato: None declared, Nobuhiko Kajio: None declared, Yasushi Kondo: None declared, Hiroaki Taguchi: None declared, Yuko Kaneko AbbVie, Asahikasei, Astellas, Ayumi, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai, Eisai, Eli Lilly, Hisamitsu, Jansen, Kissei, Pfizer, Sanofi, Takeda, Tanabe-Mitsubishi and UCB.