fetching data ... 
Background: There is a critical unmet need for effective, steroid-sparing therapies for the treatment of dermatomyositis (DM), a severe idiopathic inflammatory myopathy (IIM) characterized by a hallmark cutaneous eruption, progressive muscle weakness, and varying degrees of systemic organ involvement. Current standard-of-care therapies fail to achieve high levels of clinical response in the majority of patients and do not reliably facilitate tapering of oral corticosteroids (OCS) [1]. Even low-dose OCS use is associated with an increased risk of clinically meaningful toxicities, highlighting the importance of tapering to the lowest possible dose or discontinuing OCS altogether [2]. Brepocitinib is an investigational, first-in-class, oral, selective inhibitor of TYK2 and JAK1 administered once daily. In the 52-week, randomized, placebo-controlled, Phase 3 VALOR trial (NCT054372263) in DM patients with active skin and muscle disease despite standard therapies, brepocitinib 30 mg demonstrated statistically significant benefit on the primary efficacy endpoint (mean Total Improvement Score [TIS] at Week 52) and key secondary endpoints across multiple distinct disease domains alongside improved corticosteroid tapering [3]. VALOR provides an opportunity to assess the clinical efficacy of brepocitinib 30 mg on achievement of clinical response endpoints that also require sustained corticosteroid tapering, and to assess the efficacy of brepocitinib among participants with varying baseline OCS doses.
Objectives: To evaluate clinical response endpoints at one year, both alone and in combination with stringent corticosteroid tapering requirements, and to evaluate achievement of combined clinical response and corticosteroid tapering among subgroups of participants by baseline OCS dose.
Methods: VALOR was a 52-week, multicenter, double-blind, randomized, placebo-controlled Phase 3 trial conducted at 90 sites across 20 countries that randomized DM patients with active skin and muscle disease 1:1:1 to receive once-daily oral brepocitinib 30 mg, brepocitinib 15 mg, or placebo in combination with standard therapies. For participants receiving OCS at baseline, tapering to 5 mg/day of prednisone-equivalent dosing was required unless clinical worsening occurred; tapering below 5 mg/day was encouraged at investigator discretion. For this analysis, all clinical responses were assessed at Week 52, while OCS dose requirements were assessed at both Weeks 48 and 52 to ensure sustained corticosteroid tapering. Moderate (TIS ≥ 40) and major (TIS ≥ 60) clinical responses, as well as moderate (TIS ≥ 40) clinical response combined with a requirement for no more than minimal OCS use (OCS ≤ 2.5 mg/day), were ranked key secondary endpoints. Exploratory endpoints included major (TIS ≥ 60) response with no more than minimal OCS use, and moderate and major responses without any OCS use (i.e., maximum prednisone-equivalent dose 0 mg/day). Post-hoc analyses assessed achievement of moderate clinical response with no more than minimal OCS use among subgroups of participants defined by baseline OCS dose. Adjusted risk differences were assessed using the Cochran-Mantel-Haenszel method. All OCS use was reported as prednisone-equivalent dosing. Receipt of rescue therapy was imputed as nonresponse.
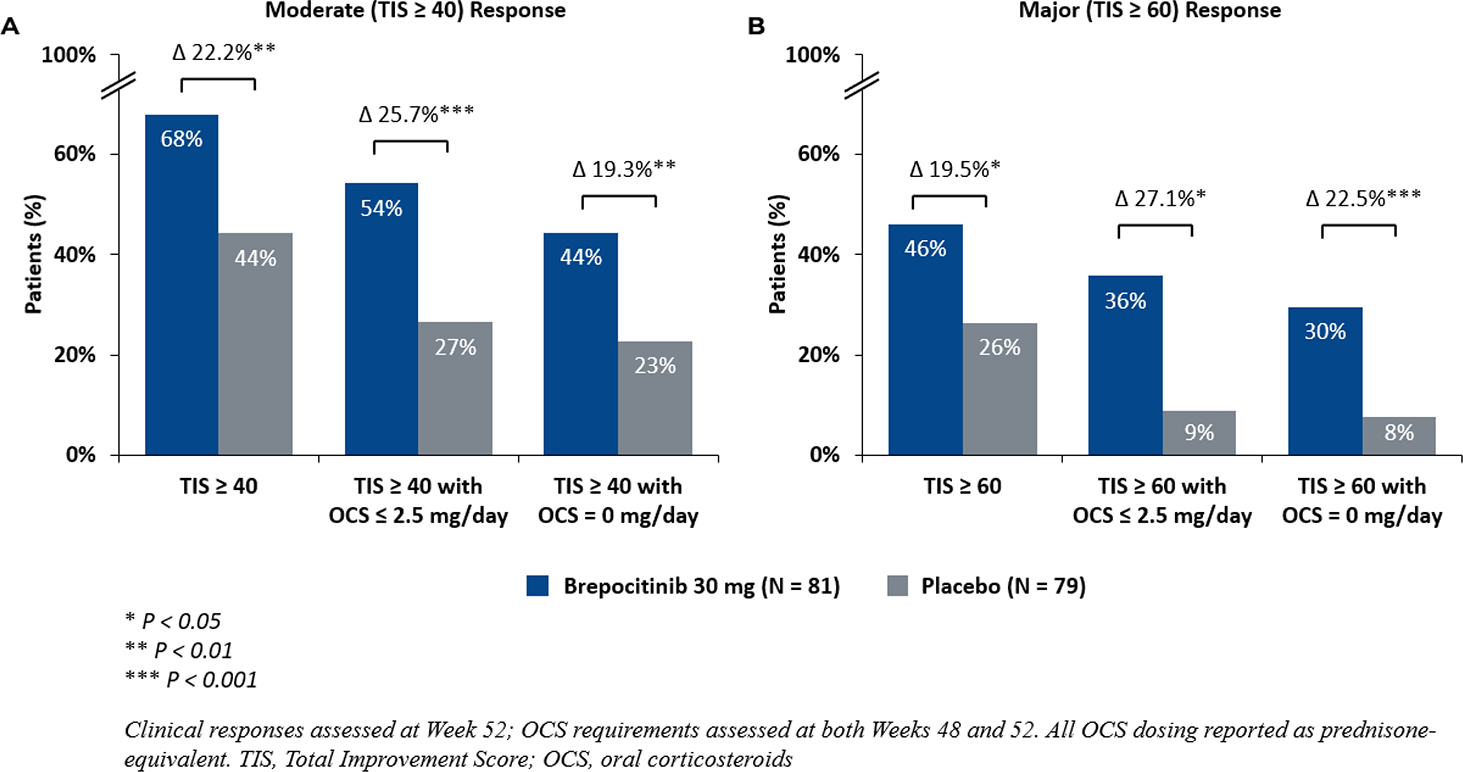
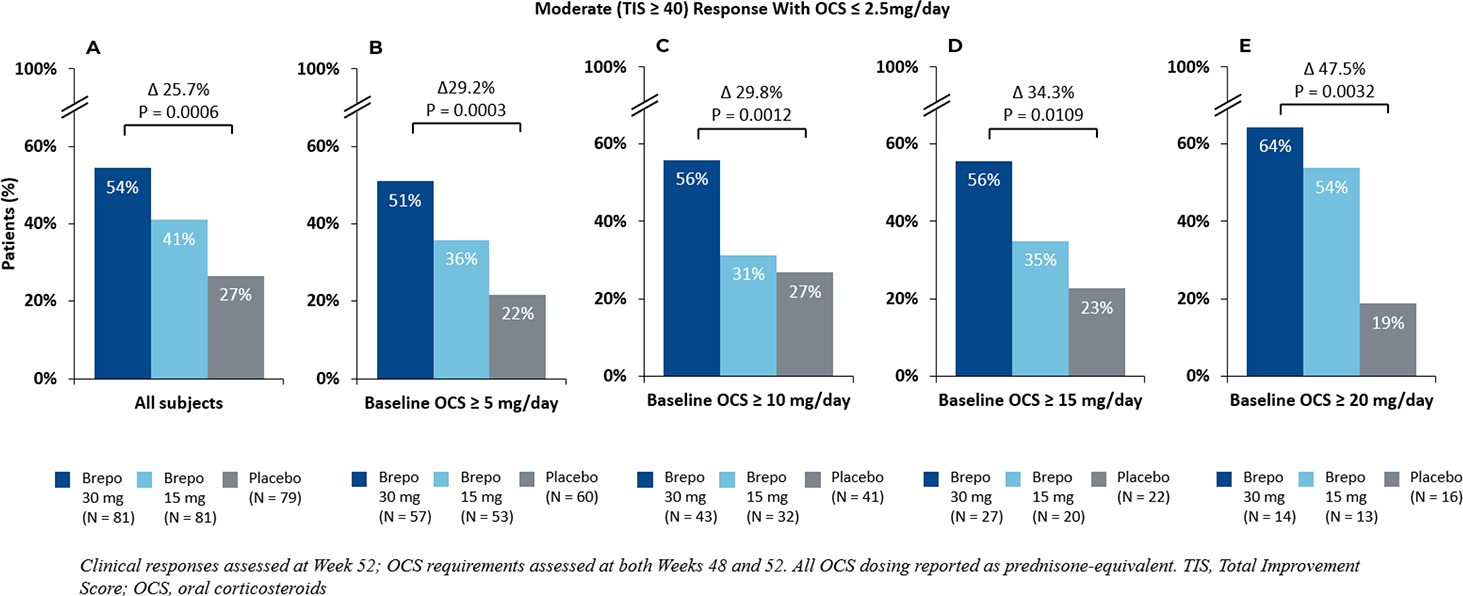
Results: 241 participants with DM and active skin and muscle disease were randomized. The majority had moderate or severe disease activity at baseline (81.3%), as reflected by a Physician Global Activity - VAS score ≥ 4 cm. The majority were also receiving OCS at baseline (75.5%), with a mean prednisone-equivalent dose of 11.4 mg/day. Brepocitinib 30 mg demonstrated superiority to placebo on the primary endpoint, mean TIS at Week 52 (least squares mean 46.5 vs. 31.2; P = 0.0006). OCS tapering to ≤ 2.5 mg/day and 0 mg/day was more frequent with brepocitinib 30 mg than placebo. Brepocitinib 30 mg demonstrated statistically significant increases in achievement of moderate and major clinical responses compared to placebo, as well as endpoints measuring combined moderate or major clinical response with sustained achievement of minimal or no OCS use at one year ( Figure 1 ). These included key secondary endpoints of moderate response (67.9% vs. 44.3%; P = 0.0040), major response (46.1% vs. 26.4%; P = 0.0126), and moderate response with OCS ≤ 2.5 mg/day (54.3% vs. 26.6%; P = 0.0006). The treatment benefit of brepocitinib 30 mg on achievement of combined clinical response and corticosteroid tapering endpoints increased with higher baseline OCS doses ( Figure 2 ). Intermediate effects were observed with brepocitinib 15 mg. Brepocitinib was generally well-tolerated, with a safety profile consistent with approved TYK2 and JAK inhibitors.
Conclusions: Brepocitinib 30 mg demonstrated benefit on combined measures of clinical response and sustained OCS tapering at one year. Treatment differences for brepocitinib 30 mg versus placebo generally increased when more stringent OCS tapering requirements were included in the endpoint definitions. Moreover, greater treatment differences for brepocitinib 30 mg versus placebo were observed among subgroups of participants with higher baseline oral corticosteroid use. These results highlight the potential for brepocitinib to deliver clinically meaningful efficacy while simultaneously reducing corticosteroid dependence. Taken together, this combined benefit supports brepocitinib as a steroid-sparing, potential therapy for patients with DM.
Moderate (TIS ≥ 40) and Major (TIS ≥ 60) Clinical Responses With and Without Oral Corticosteroid Dose Requirements For Brepocitinib 30 mg Versus Placebo at One Year
Achievement of Moderate (TIS ≥ 40) Clinical Response With Minimal or No Oral Corticosteroids (≤ 2.5mg) at One Year by Baseline Oral Corticosteroid Dose Subgroup
REFERENCES: [1] Bensimon, A. et al Amer. Col. Rheum. Convergence;1838; 2022
[2] Pujades-Rodriguez M. et al. PLoS Med. 3;17(12); 2020.
[3] Paik, J. J. et al. J. Invest. Dermatol. 145; 89; 2025
Acknowledgments: NIL.
Disclosure of Interests: Julie Paik: None declared, Eaman Alhassan: None declared, Adam Dore: None declared, Aravind Menon: None declared, Rashmi Maganti: None declared, Galina Marder: None declared, Michael Luggen: None declared, Matthew Cascino Priovant Therapeutics, Priovant Therapeutics, Kimberly DeQuattro: None declared, Anca Dinu Askanase: None declared, David R. Fernandez: None declared.