fetching data ... 
Background: Giant cell arteritis (GCA) is a large-vessel vasculitis, in which early diagnosis and treatment are essential. However, GCA presents highly heterogeneous disease manifestations and progression, posing a challenge for the early identification of severe symptoms. Genetic factors play a major role in this disease susceptibility, with the strongest and most consistent associations mapping to the human leukocyte antigen (HLA) region. Despite marked clinical heterogeneity of GCA, the contribution of HLA to specific clinical manifestations remains poorly characterized. Exploring how genetics relates to distinct clinical phenotypes may provide insights into disease mechanisms and support the development of personalized management strategies.
Objectives: The objective of this study was to identify HLA variants associated with clinical manifestations of GCA and integrate genetic biomarkers into a clinically-oriented framework.
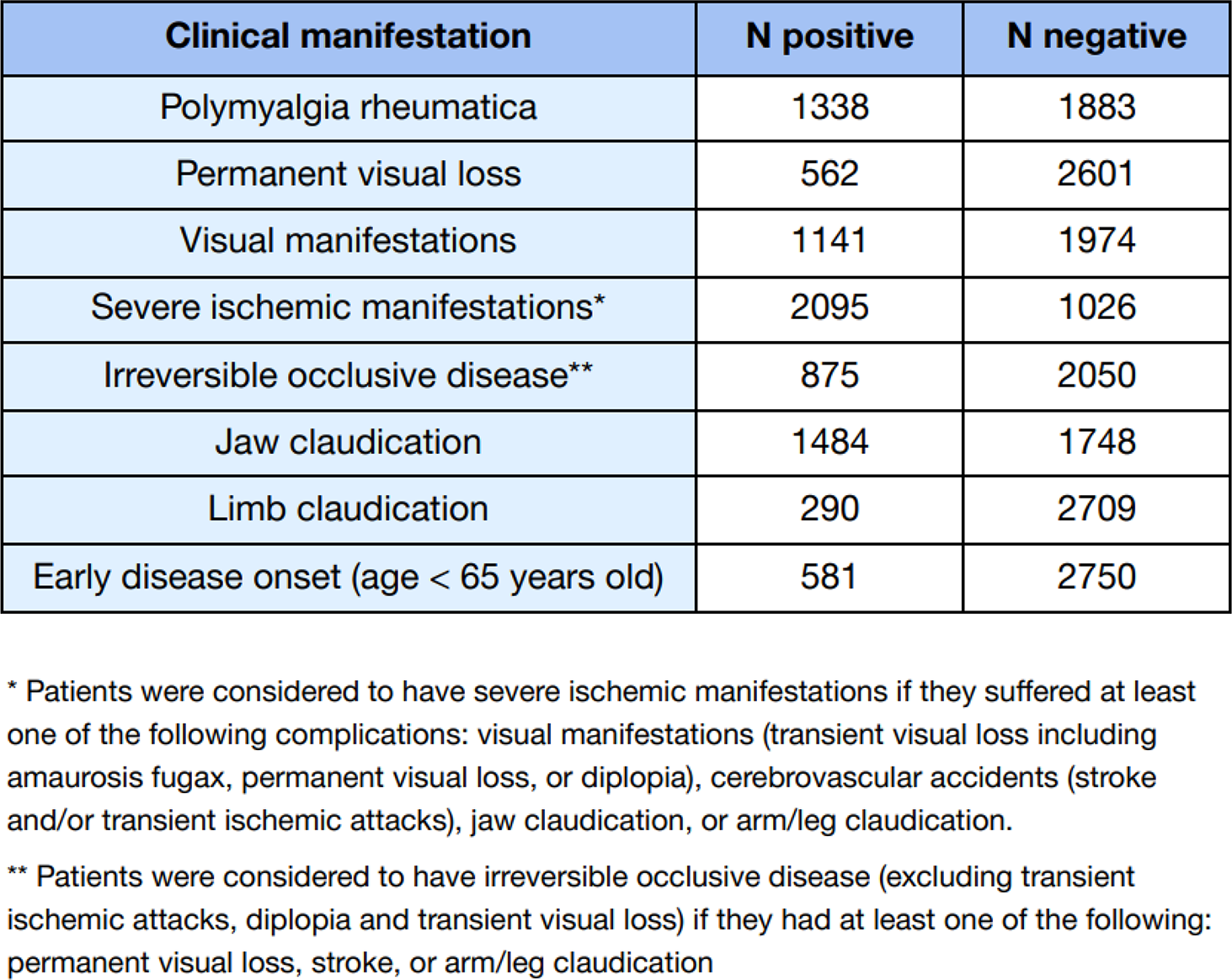
Methods: HLA genetic variants from 3,498 patients with GCA and 15,550 healthy controls were imputed from previously collected genomic data [1] using the T1DGC reference panel comprising 8961 polymorphisms (including HLA SNPs, classical alleles, and amino acid variants). Patients with GCA were stratified according to the presence of clinical phenotypes (Table 1). Logistic regression analyses were performed for each trait, adjusting for the first 10 principal components and sex, comparing: i) manifestation-positive patients and controls, ii) manifestation-negative patients and controls, and iii) patients with and without the considered manifestation. A genetic signal was considered specifically associated with a clinical manifestation if it reached genome-wide significance (p<5×10 −8 ) in the manifestation-positive versus control analysis, showed no association in the manifestation-negative versus control comparison (p>0.05), and demonstrated a modest association in the intracase comparison (p<0.005). Conditional analyses were conducted to identify independent association signals.
All manifestation-specific HLA associations, together with previously identified non-HLA genetic associations [2], were integrated using latent class analysis (LCA) to identify subgroups of patients that share genetic characteristics (genetic classes). The optimal number of classes was determined based on the Bayesian Information Criterion and class assignment certainty. Finally, the clinical profiles of the genetic classes were characterized by comparing the prevalence of clinical manifestations across classes.
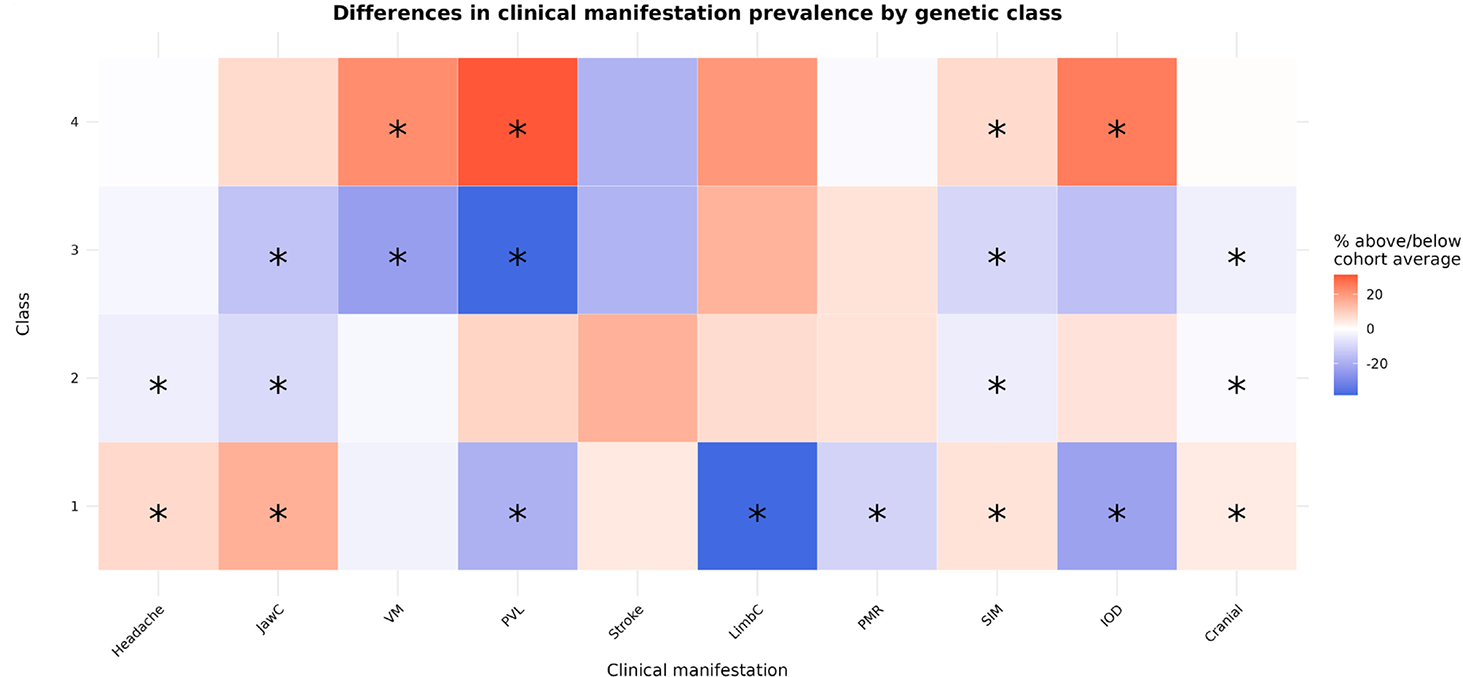
Results: Eleven significant specific associations were found with different clinical manifestations, involving 7 HLA variants and 8 clinical manifestations. Classical allele DQA1*0201 was found to be associated with an increased risk of jaw claudication (p=4.04x10 -12 ), later onset (p=4.39x10 -12 ) and cranial subtype (p=6.77x10 -11 ). In contrast, DQB1*0602 showed a protective effect for later onset (p=2.10x10 -19 ) and cranial GCA (p=9.58x10 -20 ). Independently, the rs5026743 variant also presented a protective effect for cranial GCA (p=2.72x10 -61 ). Regarding other manifestations, histidine at amino acid position 96 of the DRB1 molecule was found to confer protection specifically in patients with polymyalgia rheumatica (p=7.15x10 -15 ). Other associations were identified with visual manifestations (rs204993, p=1.42x10 -10 ), permanent visual loss (rs9275602, p=1.21x10-8), irreversible occlusive disease (rs9275602, p=1.59x10 -10 ) and severe ischemic manifestations (rs3130286, p=5.97x10 -16 ). LCA integrating 7 HLA and 7 non-HLA genetic variants showed that genetic predisposition for clinical manifestations of GCA could be robustly summarized into 4 genetic classes, with 91.2% of individuals showing a predominant class with >90% certainty. GCA genetic classes showed significant differences in several clinical manifestations (Figure 1). Class 1 (n=853) showed a cranial-predominant profile, with higher prevalence of jaw claudication, headache, and severe ischemic manifestations. Class 2 (n=1,292) exhibited a heterogeneous pattern of cranial and extracranial features. Class 3 (n=516) displayed an extracranial-leaning profile, characterized by higher prevalence of polymyalgia rheumatica and limb claudication, and reduced visual manifestations. Class 4 (n=809) was enriched for ischemic features, including permanent visual loss, comprising a potentially high-risk genetic subgroup.
Conclusions: HLA genetic variation contributes to the clinical heterogeneity of giant cell arteritis by influencing susceptibility to specific disease features. Integration of manifestation-specific genetic associations identified four genetic classes with distinct clinical profiles. These results may facilitate the clinical translation of genetic advances in GCA. In particular, this study identified a high-risk genetic subgroup (class 4) characterized by severe ischemic and visual manifestations that are not necessarily preceded by milder or more easily detectable symptoms, and which,therefore, may benefit from closer monitoring and targeted follow-up strategies, pending validation in independent cohorts. Altogether, these results highlight the potential of integrating genetic biomarkers to support the development of more precise, genetically-informed approaches to patient stratification and management in GCA.
Clinical characteristics of the cohort of patients with giant cell arteritis.
Table 1.
Distribution of clinical manifestations by genetic class, shown as deviation from the cohort mean prevalence. *Significant correlation of the prevalence of the manifestation when comparing a specific class against all others (FDR < 0.05). JawC, jaw claudication; LimbC, limb claudication; IOD, irreversible occlusive disease; PMR, polymyalgia rheumatica; PVL, permanent vision loss; SIM, severe ischemic manifestations; VM, visual manifestations.
REFERENCES: [1] Borrego-Yaniz G, et al. Lancet Rheumatol. 2024; 6(6):e374-83.
[2] Borrego-Yaniz G, et al. Ann Rheum Dis. 2025; 84:386-7.
Acknowledgments: NIL.
Disclosure of Interests: None declared.