fetching data ... 
Background: For patients with psoriatic arthritis (PsA), starting early effective treatment with disease-modifying drugs (DMARDs) is important to prevent irreversible joint damage and reduce disease burden. However, response rates of DMARDs remain relatively modest, and many patients cycle through therapies before reaching minimal disease activity (MDA). Creating individualised treatment guidelines that compare predicted responses to different DMARDs could help shorten the time to remission.
Objectives: To combine metabolomics and clinical data to develop models that predict individual treatment response to tofacitinib versus methotrexate in treatment-naïve patients (DMARD-naïve) or to add-on tofacitinib versus add-on etanercept in patients failing current treatment with a csDMARD.
Methods: Baseline metabolomics and clinical data from the TOFA-PREDICT trial discovery cohort (n=80) were used: 40 DMARD-naïve (DN) PsA patients and 40 PsA patients who previously failed DMARD therapy (DMARD-failure; DF) [1]. DN patients were randomised 1:1 to tofacitinib (TOFA) or methotrexate (MTX). DF patients continued their csDMARD and were randomised (1:1) to add-on TOFA or etanercept (ETN). Treatment response was defined as achieving Minimal Disease Activity (MDA) at week 16. Targeted metabolomics assays covering signalling lipids and amines, and a global untargeted metabolomics assay were performed [2-4]. Missing values were imputed using QRILC on log-transformed data [5]. Predictive metabolomic and clinical variables were selected using XGBoost and sPLS-DA (in the full cohort and treatment subgroups). Selected predictors were used, either directly or after dimensionality reduction using PCA, in three types of individualised treatment-effect prediction models using Ridge regression. Model development and tuning used double-loop leave-one-out cross-validation (CV). Performance estimation included an additional full-process 10-fold CV (including selection and training within each fold).
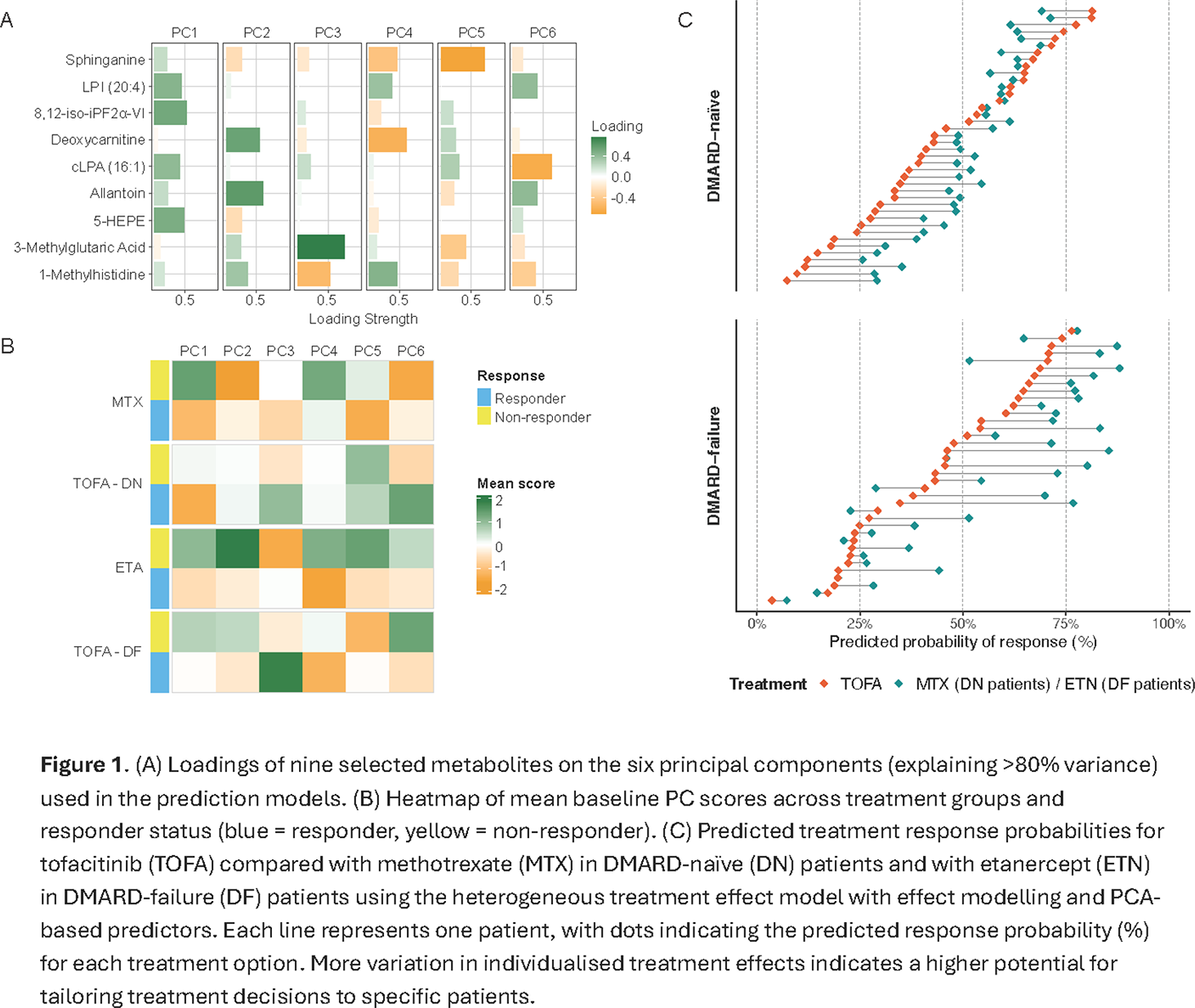
Results: Overall, 50% of patients achieved MDA at week 16. Nine metabolites (1-Methylhistidine, 3-Methylglutaric Acid, Deoxycarnitine, Allantoin, cLPA (16:1), LPI (20:4), 5-HEPE, 8,12-iso-iPF2α-VI isoprostane, Sphinganine) and one clinical variable (HAQ) were selected as predictors of treatment response. Selected metabolites include, among others, signaling lipid mediators, involved in signaling events including inflammatory processes, and markers associated with oxidative stress. The heterogeneous treatment effect model with risk modelling (HTE-risk) with PCA-derived predictors (Figure 1A-B) was the best performing approach (AUC 0.87 in the final model; mean AUC 0.78±0.18 in full-process 10-fold cross-validation; Table 1). The HTE model with effect modelling (HTE-effect) is the most flexible model in obtaining treatment-specific predictions. Although this HTE-effect model showed slightly lower discrimination (lower AUC), it produced greater separation between predicted responses for the available treatment options (Figure 1C). This is particularly helpful when making treatment decisions. This individual treatment effect varied from a 16% higher to a 24% lower predicted effect of TOFA compared to MTX in DN patients and from 19% higher to 42% lower predicted effect of TOFA compared to ETN in DF patients.
Conclusions: Baseline metabolomic signatures, together with HAQ, showed promise for predicting treatment response in PsA and for supporting individualized treatment selection. The HTE-effect model could identify relevant differences in predicted response between treatment options at the individual level. This could help physicians in choosing between treatment options. Several of the selected metabolites are linked to inflammatory processes. Together with HAQ, these markers suggest that baseline inflammatory activity and metabolic stress could contribute to achieving MDA. The predictors and models require further validation in external cohorts before clinical implementation.
Performance of homogeneous and heterogeneous treatment effect models
| Analysis | Approach | HOM | HTE - Risk | HTE - Effect |
|---|---|---|---|---|
| Final model | Direct | 0.78 | 0.83 | 0.77 |
| PCA | 0.79 | 0.87 | 0.83 | |
| Full-process 10-fold CV | Direct | 0.75 ± 0.16 | 0.72 ± 0.15 | 0.74 ± 0.15 |
| PCA | 0.75 ± 0.18 | 0.78 ± 0.18 | 0.72 ± 0.17 |
Values are AUC-ROC. Final model rows report AUCs using all data once. Full-process 10-fold CV rows show mean ± SD AUCs from a full 10-fold CV, with predictor selection and model training repeated within each fold. HOM = homogeneous treatment effect model; HTE-Risk = heterogeneous treatment effect model with risk modelling; HTE–Effect model = HTE model with effect modelling.
REFERENCES: [1] Kleinrensink, Nienke J., et al. “TOFA-PREDICT study protocol: a stratification trial to determine key immunological factors predicting tofacitinib efficacy and drug-free remission in psoriatic arthritis (PsA).” BMJ open 12.10 (2022): e064338.
[2] Noga MJ, Dane A, Shi S, et al. Metabolomics of cerebrospinal fluid reveals changes in the central nervous system metabolism in a rat model of multiple sclerosis. Metabolomics. 2012;8:253–63. doi: 10.1007/s11306-011-0306-3.
[3] Yang W, Schoeman JC, Di X, et al. A comprehensive UHPLC-MS/MS method for metabolomics profiling of signaling lipids: Markers of oxidative stress, immunity and inflammation. Analytica Chimica Acta. 2024;1297:342348. doi: 10.1016/j.aca.2024.342348.
[4] Zhu P, Dubbelman A-C, Hunter C, et al. Development of an Untargeted LC-MS Metabolomics Method with Postcolumn Infusion for Matrix Effect Monitoring in Plasma and Feces. J Am Soc Mass Spectrom. 2024;35:590–602. doi: 10.1021/jasms.3c00418.
[5] Karu N, Kindt A, van Gammeren AJ, et al. Severe COVID-19 Is Characterised by Perturbations in Plasma Amines Correlated with Immune Response Markers, and Linked to Inflammation and Oxidative Stress. Metabolites. 2022;12:618. doi: 10.3390/metabo12070618.
[6] Wei R, Wang J, Su M, Jia E, Chen S, Chen T, Ni Y. Missing value imputation approach for mass spectrometry-based metabolomics data. Scientific reports. 2018 Jan 12;8(1):663.
Acknowledgments: NIL.
Disclosure of Interests: Mieke L. M. Bentvelzen: None declared, Wei Yang: None declared, Yu Zhang: None declared, Alida Kindt: None declared, Amy C. Harms: None declared, Julia Spierings research grants from Boehringer Ingelheim and Miltenyi Biotec, Amin Herman: None declared, Shasti C. Mooij: None declared, Lydia G. Schipper: None declared, Harald E. Vonkeman AstraZeneca, Lilly, Pfizer, Abbvie, Novartis, Pfizer, UCB, Johnson and Johnson, Alphasigma, Galapagos and Boehringer Ingelheim, simone vreugdenhil: None declared, Simon C. Mastbergen ReumaNederland LLP-9, Thomas Hankemeier: None declared, Paco Welsing: None declared.