fetching data ... 
Background: Lupus nephritis (LN) is one of the most severe manifestations of SLE, affecting approximately 40% of patients. Despite aggressive immunosuppressive regimens combining corticosteroids with cyclophosphamide (CYC), mycophenolate mofetil (MMF), or rituximab (RTX), complete remission (CR) rates vary between 50-70% at 12 months. This heterogeneity in treatment response is unpredictable and no validated tool exists for risk stratification at diagnosis, making management of LN patients challenging. Early identification of patients at high risk of treatment failure would enable clinicians to tailor treatments and monitoring.
Objectives: Using machine learning (ML) approaches, this study aimed to develop a simple score based on routine baseline parameters to predict the probability of CR at 12 months.
Methods: We conducted a retrospective single-center study of LN cases from a tertiary university hospital between 2006 and 2023. Inclusion criteria comprised biopsy-proven class III or IV active LN (according to the ISN/RPS classification [1]) and a minimum follow-up of 12-month. The primary outcome was CR at 12 months, defined according to the EULAR criteria as proteinuria <0.5g/24h with stable renal function. We first performed univariate screening of baseline variables encompassing demographics, clinical parameters, laboratory values, histological features, and treatment modalities to identify candidate predictors associated with CR. For ML analysis, the cohort was split into training (70%, n=131) and validation (30%, n=55) sets using stratified sampling. Different ML models (random forest, Ridge regression, gradient boosting) were trained to predict CR, and their performance was assessed using area under the ROC curve in the held-out validation set. Based on the top predictors identified by ML, a simplified score ranging from 0 to 5 was derived, and subsequently evaluated for performance in the validation cohort.
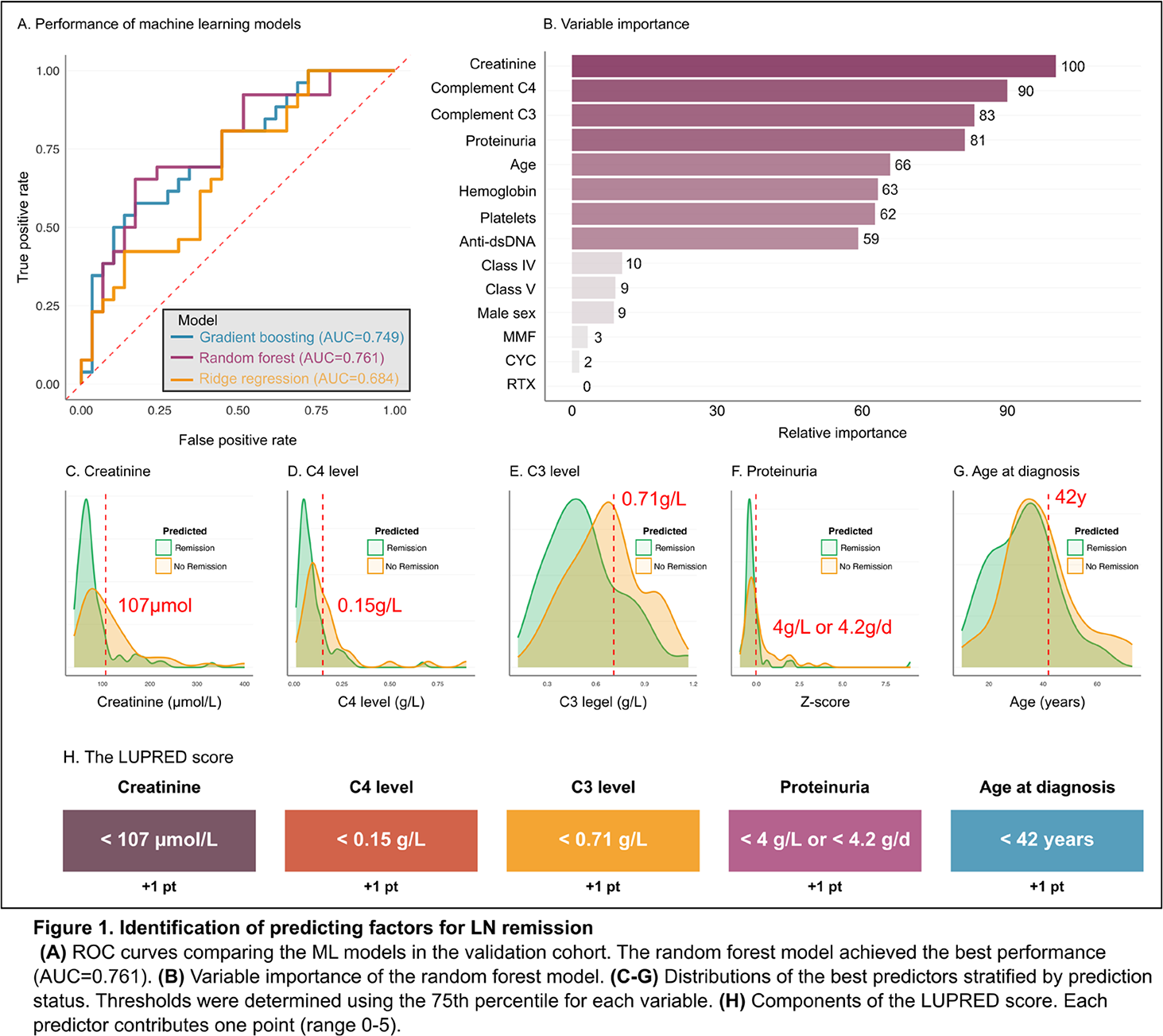
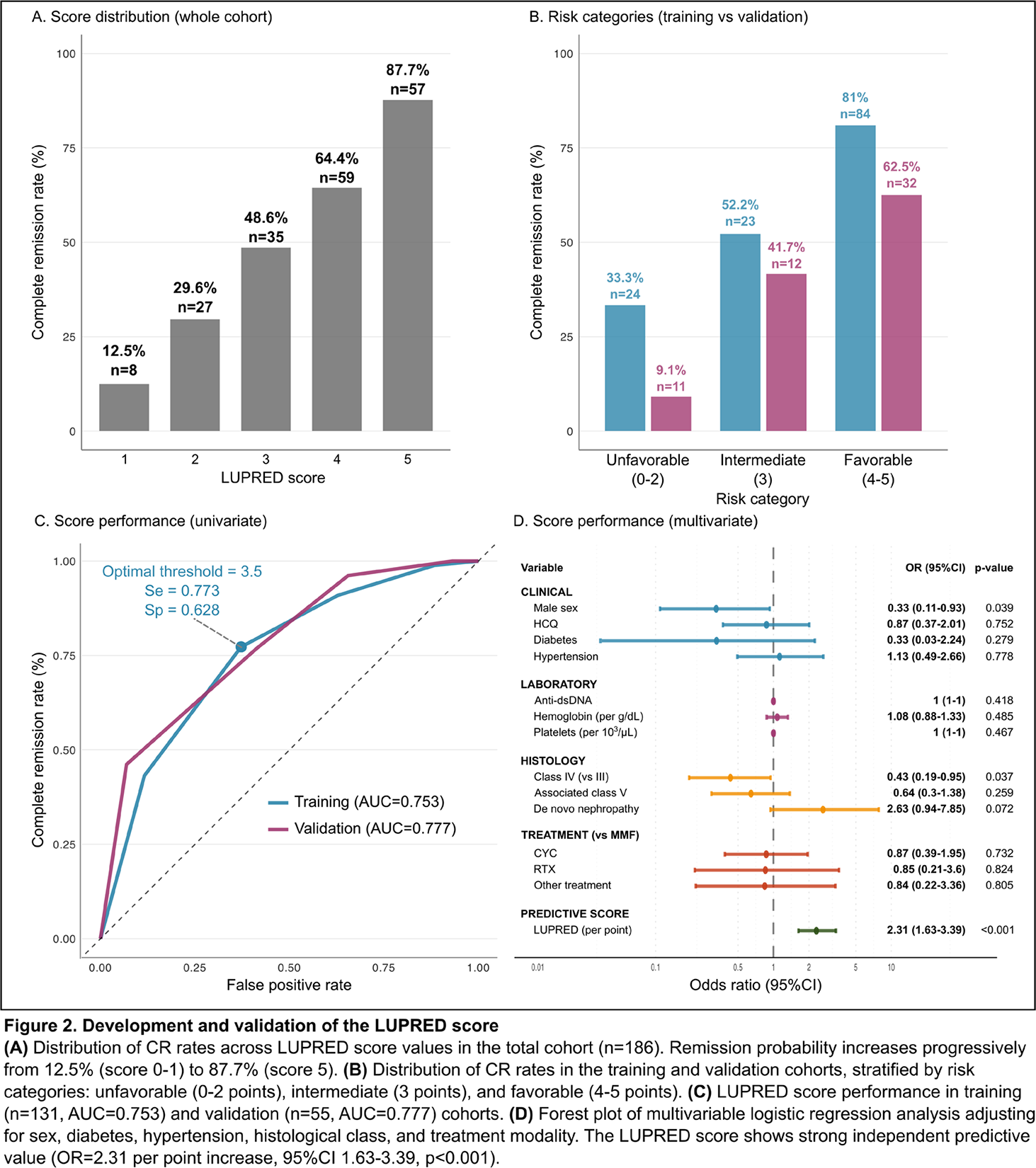
Results: A total of 186 patients were included, of whom 156 female cases (84%). The median age at LN diagnosis was 34 years (IQR 25-42 years). According to the ISN/RPS histological classification, class III and IV LN were equally represented (n=93, 50% each), and 68 cases (37%) had associated class V features. Induction therapy consisted of MMF (n=83, 45%), CYC (n=71, 38%), RTX (n=16, 8.6%), and other regimens (n=16, 8.6%). Overall, 114 patients (61.2%) had achieved CR at 12 months. Univariate analyses identified 15 variables significantly associated with CR (p<0.05), including age, sex, diabetes, hypertension, BMI, hydroxychloroquine use, class III versus IV histology, initial creatinine, initial proteinuria, C-reactive protein, C3 and C4 complement levels. Using these variables, the random forest model achieved the best predictions of CR with AUC=0.761 ( Figure 1A ). Initial creatinine, C4 and C3 complement levels, proteinuria, and age at biopsy as the top-five predictors of CR ( Figure 1B ). These top-filve predictors were binarized using the 75 th percentile of each variable ( Figure 1C-G ), and used to construct the LUPRED score, to estimate the baseline probability of achieving CR at 12 months. Each favorable prognostic factor contributes 1 point (age<42 years, creatinine<107 μmol/L, proteinuria<4.0 g/L or <4.2 g/24h, C3 level<0.71 g/L, and C4 level<0.15 g/L), with a resulting score ranging from 0 to 5 ( Figure 1H ). Score distribution showed a clear gradient of CR probability, from 87.7% for patients with 5 pts down to 12.5% for those with ≤1 pts ( Figure 2-AB ). We then evaluated the LUPRED score in the training cohort, demonstrating an AUC of 0.753, yielding a sensitivity of 77.3% and a specificity of 62.8% at the 3.5 optimal cutoff ( Figure 2C ). The performance in the test cohort was comparable with an AUC of 0.777. When included into multivariable logistic regression adjusting for sex, diabetes, hypertension, histological class, and treatment modality, the LUPRED score maintained strong independent predictive value with OR=2.31 per point increase (95%CI 1.63-3.39, p<0.001), confirming its robustness beyond classical confounders ( Figure 2D ).
Conclusions: We developed LUPRED, a 5 variable score predicting CR in proliferative LN. The score demonstrates excellent discrimination with clinically meaningful prognostic stratification. Its reliance on routine baseline parameters facilitates immediate implementation for treatment personalization. Validation in independent multicenter cohorts is required prior to clinical implementation.
REFERENCES: [1] Bajema IM, Wilhelmus S, Alpers CE, Bruijn JA, Colvin RB, Cook HT, et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. avr 2018;93(4):789-96.
Acknowledgments: NIL.
Disclosure of Interests: Clarisse Doutriaux: None declared, Alexis Chambost: None declared, Marie Robert: None declared, Quitterie Reynaud: None declared, Fitsum Guebre-Egziabher: None declared, PASCAL SEVE Abbvie, Fresenius Kabi, GlaxoSmithKline, Lilly, Novartis, Pfizer and Sanofi, Laetitia Koppe: None declared, Laurent Perard: None declared, Maud Rabeyrin: None declared, Ludovic Trefond: None declared, Arnaud Hot: None declared, Thomas Barba GSK, AstraZeneca.