fetching data ... 
Background: Sjögren’s disease (SjD) is a systemic autoimmune disorder characterized by marked clinical and biological heterogeneity. Defining disease subgroups with distinct tissue-level pathobiological features may advance understanding of disease mechanisms and support the development of targeted therapeutic approaches.
Objectives: Our aims were (i) to identify potential subgroups of patients with SjD in an explorative study by proteome analysis of minor salivary gland (MSG) tissues, and (ii) to determine clinical and molecular differences between subgroups.
Methods: Flash frozen minor salivary glands (MSG) from 18 SjD patients, fulfilling the 2016 ACR/EULAR classification criteria (1) were analyzed, and their clinical data were collected. This included demographic, histological, imaging, functional, laboratory parameters and clinical characteristics such as age, gender, focus score, number of germinal centers (GC), salivary gland ultrasound scores (SGUS), Schirmer’s test, unstimulated salivary flow (USF) test, presence of autoantibodies, ESSDAI and ESSPRI score. Proteome analysis of the MSG tissues was performed by tandem mass spectrometry. Proteins were identified and quantified using the Spectronaut software. Principal component analysis (PCA) was performed based on log2-transformed Spectronaut intensities (SI). Bayes test was applied to identify differentially expressed proteins (log2 FC≥ 1, p-adj ≤0.05) between clusters. Pathway enrichment analysis for Reactome pathways and protein protein interaction (PPi) network analysis were performed on differentially expressed proteins using the STRING database. A second independent cohort of 23 SjD patients was included for immunofluorescence validation of selected target proteins in formalin-fixed paraffin-embedded (FFPE) MSG tissue sections. To reflect the three groups identified in proteomic analysis, patients from the second cohort were stratified into three groups based on focus score and USF (group 1 - focus score>2; USF<0,1 ml/min; group 2 - focus score 1-2; USF <0,8 ml/min; group 3 - focus score<1,5; USF>0,13 ml/min).
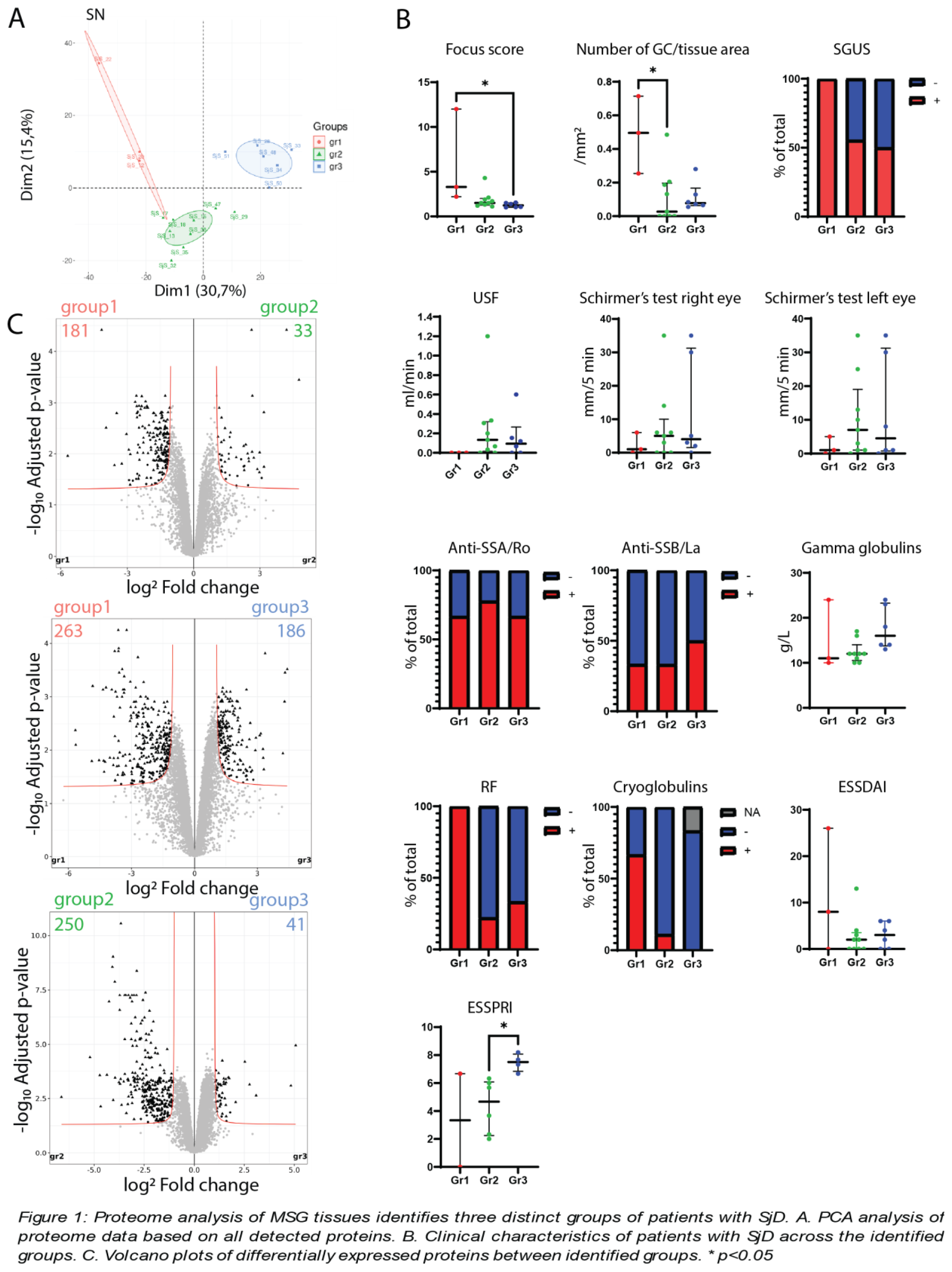
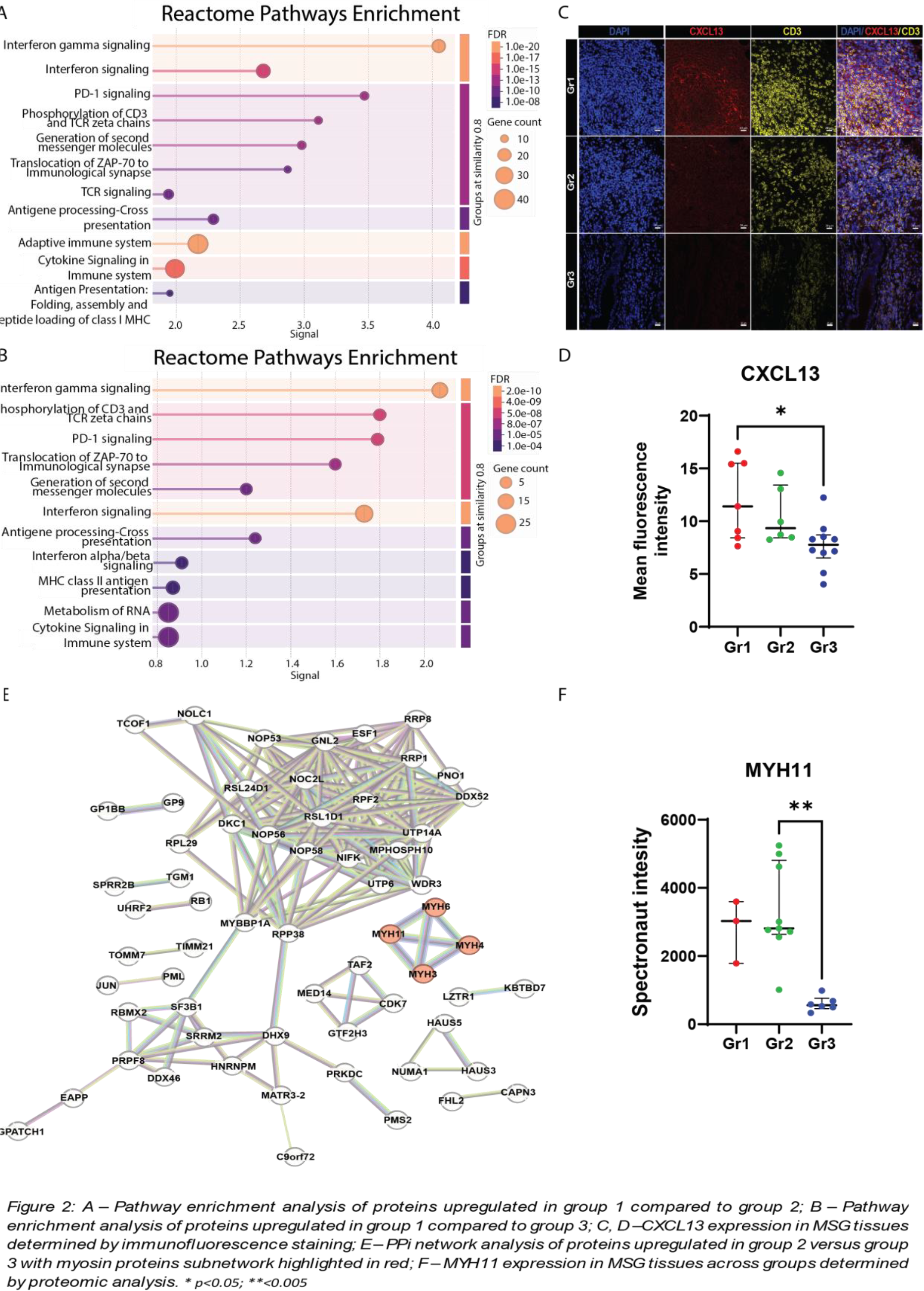
Results: We detected 8192 proteins in MSG tissues by proteome analysis. PCA identified three separate groups of patients with SjD (Figure 1A). Patients from group 1 (n=3) had significantly higher focus scores and number of GC per tissue area and a lower USF when compared to groups 2 (n=9) and 3 (n=6). In addition, the percentage of patients testing positive in SGUS was higher in group 1. Furthermore, group 1 had a higher percentage of patients positive for rheumatoid factor (RF) and cryoglobulins (Figure 1B). Groups 2 and 3 were clinically similar, however differential protein expression analysis highlighted the molecular differences between all three groups. In cluster 1, 181 proteins were upregulated and 33 were downregulated compared to cluster 2, and 263 proteins were upregulated and 186 downregulated compared to cluster 3. In cluster 2, 250 proteins were upregulated and 41 were downregulated when compared to cluster 3 (Figure 1C). Pathway enrichment analysis of proteins upregulated in group 1 compared to groups 2 (Figure 2A) and 3 (Figure 2B) identified IFN signaling, antigen presentation and T cell activation as key dysregulated pathways in group 1. Consistently, group 1 exhibited the highest expression of the IFN-induced chemokine CXCL13, detected by immunofluorescence in MSG tissues from second cohort of patients (Figure 2C, D). PPi network analysis of upregulated proteins in group 2 compared to group 3 showed a subnetwork of class II myosin heavy chain proteins, key mediators of muscle contractility (Figure 2E). Expression of MYH11, which servs as a functional marker of myoepithelial cells (2), was additionally shown to be downregulated in group 3 compared to groups 1 and 2 (Figure 2F), potentially suggesting to myoepithelial cell dysregulation in group 3.
Conclusions: SjD patients in our cohort clustered in 3 groups based on MSG proteomes. Group 1 clinically showed most sever glandular damage and molecularly the highest immune dysregulation. Groups 2 and 3 were clinically similar, but molecularly different, with group 3 showing a downregulation of MYH11 expression potentially pointing out to myoepithelial cell dysregulation.
REFERENCES: [1] Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data‐Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017;69(1):35-45.
[2] Prater MD, Petit V, Alasdair Russell I, Giraddi RR, Shehata M, Menon S, et al. Mammary stem cells have myoepithelial cell properties. Nat Cell Biol. 2014;16(10):942-50, 1-7.
Acknowledgments: NIL.
Disclosure of Interests: Neža Štucin: None declared, Matthias Brunner: None declared, Katja Perdan Pirkmajer: None declared, Alojzija Hočevar: None declared, Jože Pižem: None declared, Britta Maurer Unrelated to this specific study, BM declares lecturing fees from Boehringer Ingelheim, GaxoSmithKline, Novartis, Otsuka, and Merck Sharpe & Dohme, Lilly, Unrelated to this specific study, BM declares she has been on an advisory board for Janssen and Boehringer, Unrelated to this specific study, BM declares consulting fees from Novartis, Boehringer Ingelheim, Janssen-Cilag, and GaxoSmithKline, Unrelated to this specific study, BM declares research grants from AbbVie, Protagen, and Novartis Biomedical Research., Saša Čučnik: None declared, Polona Zigon: None declared, Kerstin Klein: None declared.