fetching data ... 
Background: Sjögren’s disease (SjD) is a systemic autoimmune disease with diverse clinical presentation. Heterogeneity within SjD has been described through the presence or absence of the Ro autoantibody. Anti-Ro negative SjD patients are underrepresented in research studies and often excluded from clinical trial recruitment. Better cellular and molecular phenotyping is necessary for improved diagnosis and stratification of SjD and the development of treatments. To address this problem, our large cohort of 50 controls, 87 anti-Ro - SjD patients, and 116 anti-Ro + SjD patients includes substantial representation from both main serological subphenotypes. Here, we leveraged single-cell RNA sequencing (scRNA-seq) with surface protein profiling of ~2 million peripheral blood mononuclear cells (PBMCs) to refine our understanding of pathogenic pathways across anti-Ro + and anti-Ro - SjD.
Objectives: To characterize SjD-associated cell populations and transcriptional signatures and examine differences between anti-Ro - and anti-Ro + SjD to uncover distinct pathogenic mechanisms underlying the two subphenotypes.
Methods: PBMCs were isolated from human subjects with SjD and healthy controls. After reviewing clinical data from the ~1700 subjects enrolled in the Oklahoma Sjögren’s Cohort, 253 subjects were selected for this study (Figure 1A). 10X Genomics Chromium scRNA-seq was performed and sequencing data were demultiplexed using the 10X Genomics Cell Ranger (v10.0) pipeline and aligned to the GRCh38 human genome. After quality control, using Seurat and scDblFinder to remove low-quality cells and doublets, a total of 2,088,744 cells were integrated and clustered. Immune cell types were manually annotated through careful reference of canonical immune cell markers. NEBULA was used for differential expression (DE) analysis of transcripts from each cell type across the different subject groups. Significantly DE transcripts were input into Ingenuity Pathway Analysis (IPA).
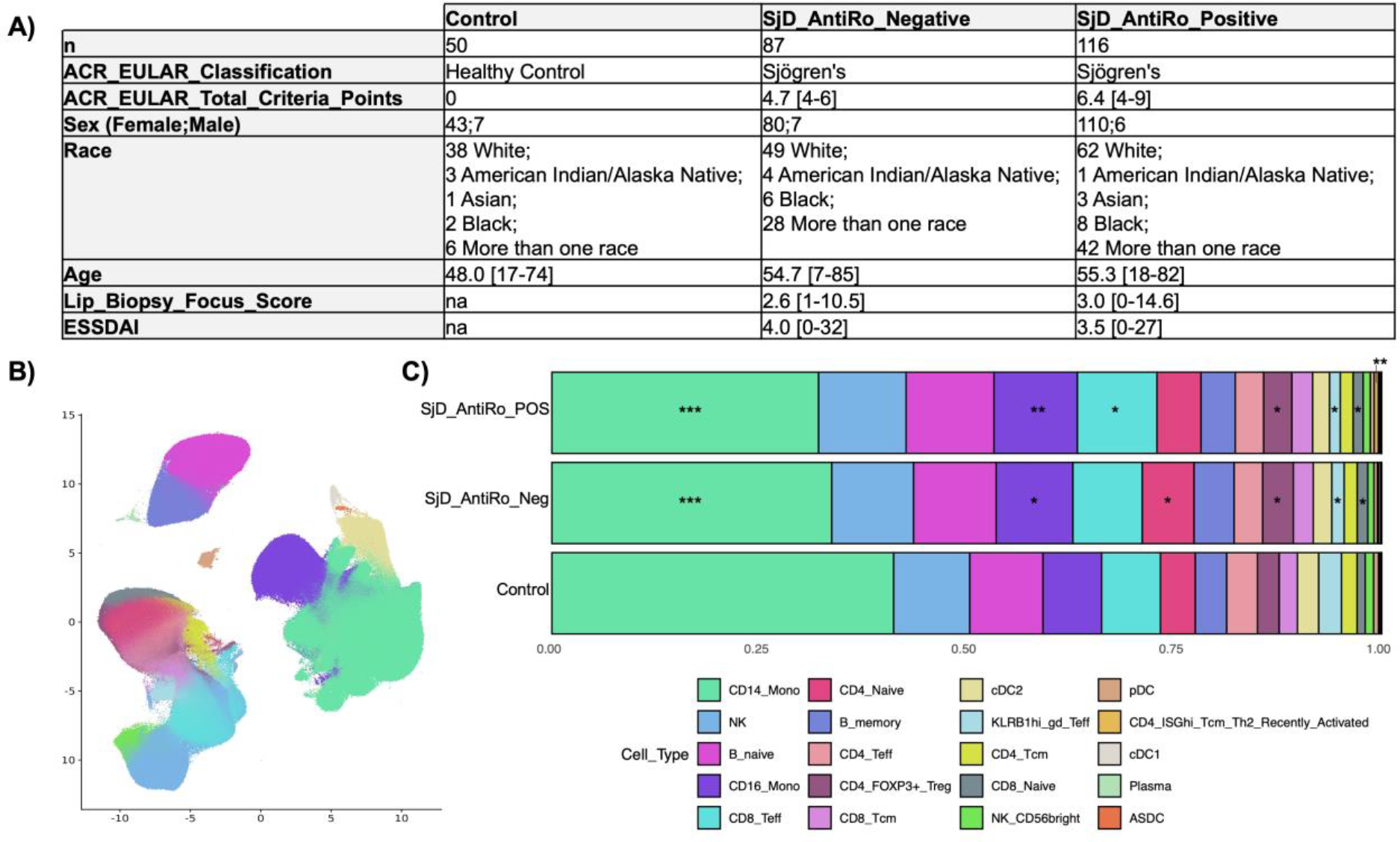
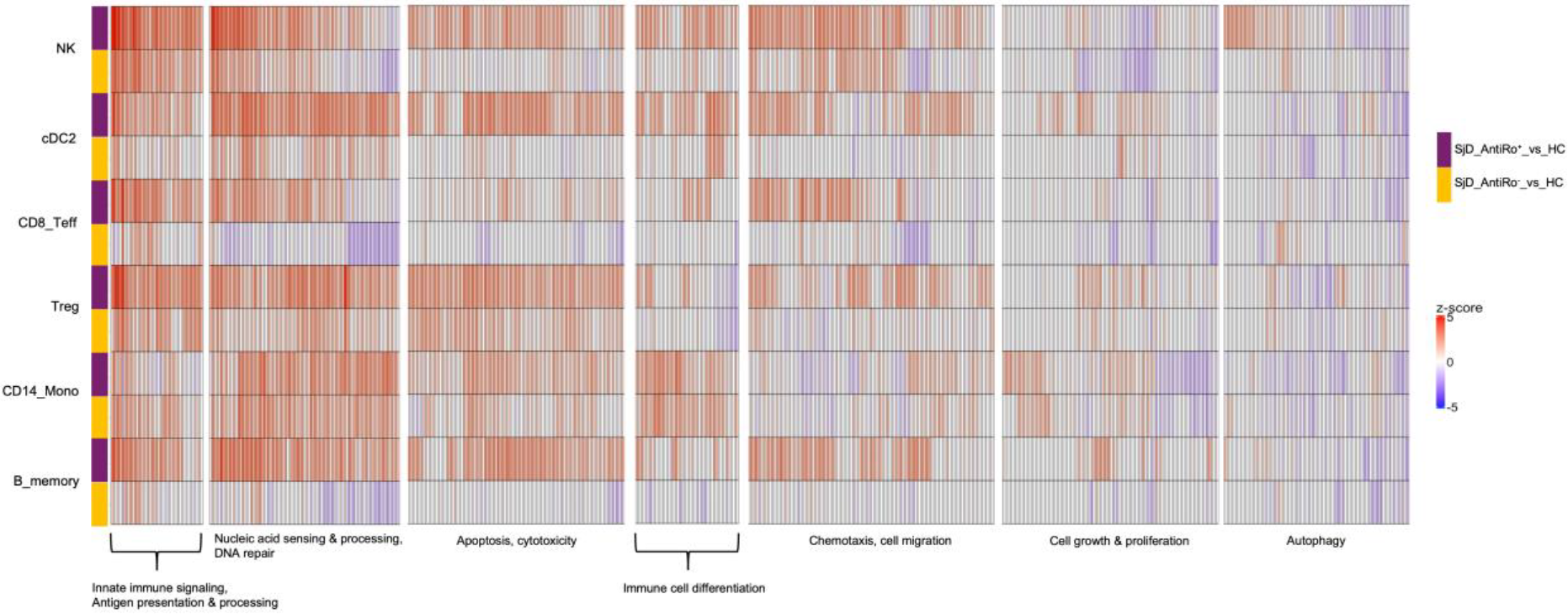
Results: Twenty total cell types were identified, capturing all major classes of immune cells in the peripheral blood (Figure 1B). Cell type proportion analyses showed reduced proportions of CD14 + monocytes and KLRB1 + γδ T cells in SjD groups compared with controls. In contrast, increased proportions were detected for CD16 + monocytes, CD8 + effector T cells, regulatory T cells (Tregs), and naïve T cells (Figure 1C). Expression changes converged to 7 major biological themes summarizing functionally related molecular pathways (Figure 2). Pathways related to innate immune signaling, antigen processing and presentation, nucleic acid sensing and processing, autophagy, apoptosis, immune cell differentiation, cell migration, and cell proliferation were dysregulated in both anti-Ro - and anti-Ro + SjD (Figure 2). Generally, anti-Ro + SjD patients showed increased dysregulations and greater numbers of dysregulated pathways than anti-Ro - SjD patients. While many pathways were broadly dysregulated across immune cell classes and shared between disease subphenotypes, some pathways demonstrated cell type- and disease subphenotype-specific activity. For example, pathways such as cGAS-STING signaling, TLR cascades, and DNA damage response showed differing activity between anti-Ro + and anti-Ro - SjD.
Conclusions: These results suggest that anti-Ro + and anti-Ro - SjD patients share many disease-associated pathways but also exhibit distinct transcriptional patterns. Immune cells exhibited dysregulations in pathways regulating immune responses, differentiation, apoptosis, and autophagy in both anti-Ro + and anti-Ro - SjD. Deeper molecular profiling of patients could help further delineate key pathways shared among all disease subphenotypes from processes specific to certain disease subphenotypes.
Characteristics of patient cohort and cell populations. A) Demographic and clinical information for the cohort (n=253). Numeric data shown as {mean [min-max]} where relevant. B) UMAP visualization of annotated cell populations. C) Cell type proportions across study groups (* p < 0.05, ** p < 0.01, *** p < 0.001 calculated from Student’s t-test.)
Cell type specific dysregulations in Anti-Ro + and Anti-Ro - SjD. Significantly DE transcripts (adjusted p<0.05) for each patient group (purple: Anti-Ro + SjD, yellow: Anti-Ro - SjD) compared to control were analyzed by IPA. Plots show upregulated (red) and downregulated (blue) pathways grouped by biological function in memory B cells, CD14+ monocytes, regulatory T cells (Treg), CD8+ effector T cells (CD8_Teff), type 2 conventional dendritic cells (cDC2), and natural killer cells (NK).
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: James Li: None declared, Bhuwan Khatri: None declared, Songyuan Yao: None declared, Marcin Radziszewski: None declared, Cherilyn Pritchett Frazee: None declared, Mandi M Wiley: None declared, Kandice L Tessneer: None declared, Christina Lawrence: None declared, Hope Christakos: None declared, Charmaine Lopez-Davis: None declared, Tommi C Taylor: None declared, Michelle L Joachims: None declared, Astrid Rasmussen Current affiliation: Boston Children’s Hospital, Received consulting fees from Immunovant Clinical Outcomes Solutions, R Hal Scofield Received consulting fees from Johnson and Johnson Innovative Medicine (formerly Janssen) and Merk Pharmaceuticals, Blake M Warner Active research agreements with Astellas Bio, Pfizer, Judith A. James Received consulting fees from GSK., Received research support from Progentec Biosciences, Joel M Guthridge: None declared, A. Darise Farris Grant/research support from Johnson and Johnson Innovative Medicine (formerly Janssen; ended 12/31/2023), Christopher J Lessard Johnson & Johnson Sjögren’s Disease Advisory Board, Johnson and Johnson Innovative Medicine (formerly Janssen; ended 12/31/2023).