fetching data ... 
Background: Rheumatology remains a constantly evolving speciality, with ever-expanding treatment modalities, including both new medication options, and increasing applications of established treatments. Axial Spondyloarthritis (AxSpA) is a type of inflammatory arthritis that typically begins in the sacroiliac joints, characterised by features of inflammatory back pain and loss of function. It is treated with intermittent non-steroidal anti-inflammatory (NSAID) use/ exercise in milder disease, with biologic treatments revolutionising the management of moderate/ severe disease (1). Prior to commencing patients on biologic/ traditional disease modifying treatments, patient education, typically delivered by nurse, is central to the treatment plan (2). Moreover, nurse-led care has been shown to be effective, and non-inferior to consultant-led care in Rheumatoid Arthritis consistently for over a decade (3, 4). Despite nurses being seen as central to care coordination, patient education and self-management support, evidence remains lacking demonstrating value that specialist nurses (including Advanced Nurse Practitioners) (ANPs) can offer patients living with AxSpA.
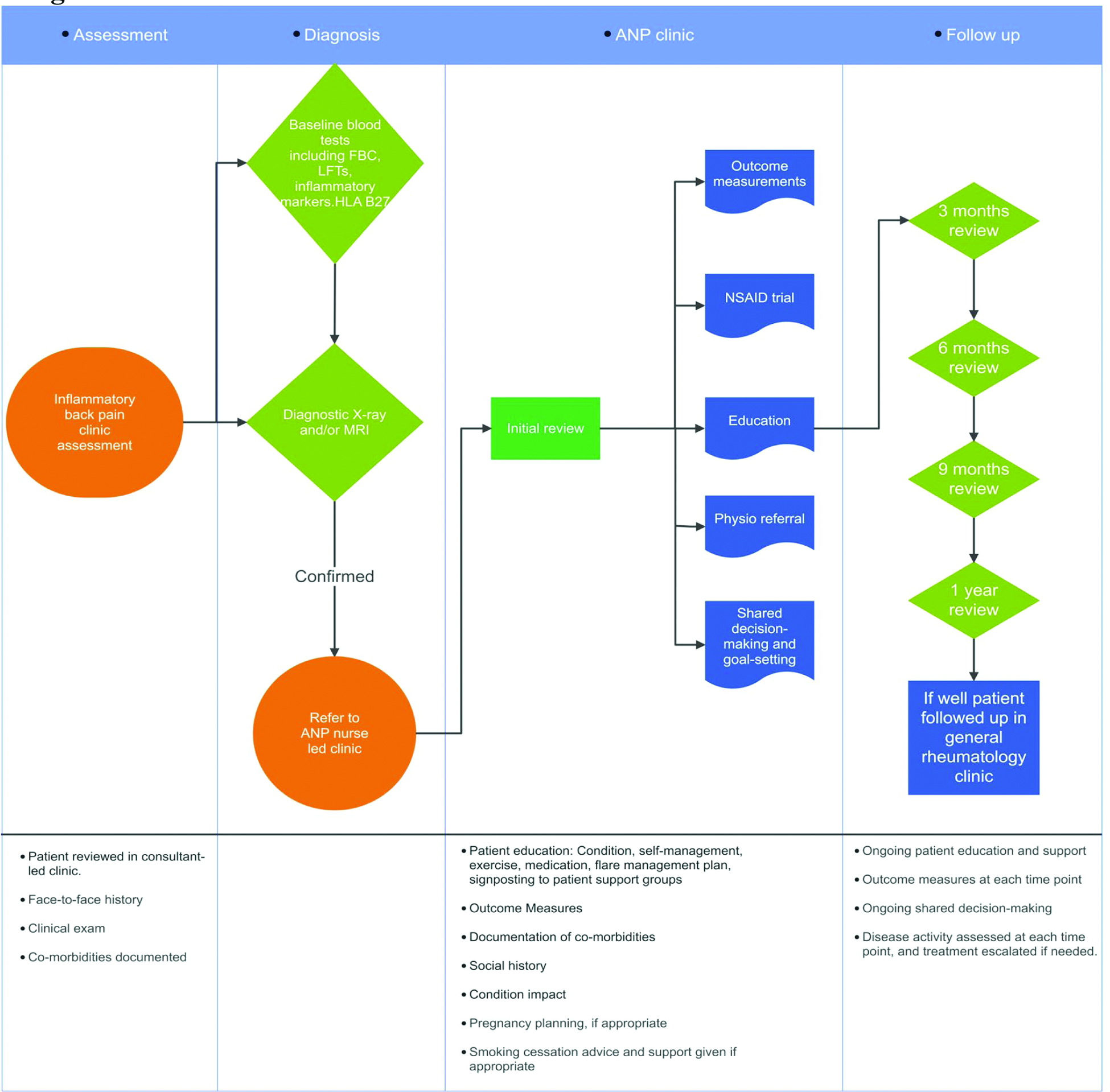
Objectives: An ANP-led pathway has been in operation since January 2025 in our department, offering 3/4 appointments to patients newly diagnosed with AxSpA across approx. 12 months to include patient reported and physical outcome measures; medication review/ change as required; physiotherapy referral (where needed) for structured exercise; health promotion and individualised patient education. The goal of the treatment pathway was to support a patient navigating year 1 post diagnosis to support patient self-management, optimise treatment and return to medical clinic for follow up once stable on treatment.
Methods: Following confirmation of inflammatory back pain symptoms, sacroiliitis via MRI/ plain film X-ray, and HLA B27 status; patients were referred to follow the ANP-led AxSpA clinic pathway for minimum 12 months post diagnosis (see Table 1). Patients were offered a face to face appointment to include medicine reconciliation; review of NSAID use; patient reported outcome measures (PROMs)(BASDAI/ BASFI/ BAS-G); physical measurements (BASMI); assessment of comorbidities (using MECC principles) to include smoking/ alcohol/ cardiovascular risk/ bone health, vaccine history and work status; education regarding condition and treatment plan, blood monitoring/ pre-biologic screening; pre-pregnancy planning; medication prescription; and physiotherapy referral. Follow up appointments were offered at minimum 4month intervals to assess ongoing disease activity, response to treatment to date, PROMs and physical assessment, willingness to consider smoking/ alcohol reduction/ vaccine uptake where needed, engagement with physiotherapy/ blood monitoring with the aim of maximising treatment response and encourage self-management.
Results: From January 2024 to December 2025, 91 newly diagnosed AxSpA patients joined the ANP-led pathway. Of these, to date, 60 have completed the minimum 3 visits, 53% are male and 55% are under 40 at diagnosis, and a further 15 were under 50. 70% reported no extra-musculoskeletal manifestations, with 17% reporting Psoriasis, 4.5% Uveitis, and 6.3% inflammatory bowel disease. 32% attended physiotherapy prior to visit 1. 68% had already trialled minimum 1 NSAID by visit 1, and 55% were starting a biologic after visit 1. Average outcome measures across 3 visits as per table 1 below. Patient education was tailored to the individual, varied across the 3 visits and included information about diagnosis, typical patient journey (including reason for physiotherapy referral and importance of stretching/ exercise in AxSpA), role of NSAIDs, reason for pre-biologic screening, medication education as appropriate, pre- conception advice as appropriate, importance of vaccines to reduce infection risk, health promotion (including MECC as above, and current work status), provision of written resources (typically on diagnosis/ medicines) and signposting to online resources (including Arthritis Ireland, Versus Arthritis and National Axial Spondyloarthritis Society (NASS) websites/ social media channels). By visit 2, 77% were prescribed biologics, with 26% requiring dose increase/ medication switch at this review. 38% reported reduction in anti-inflammatory use, and 50% had been reviewed by physiotherapy. At visit 2 BASDAI/ BASFI reported minimally clinically important difference, with BAS-G achieving by visit 3 (5). By visit 3, biologic use was 85%; anti-inflammatory use was rare in 68%; and drug persistence was 70%. At visit 2 and visit 3, patients were asked about any change in medicines taken, medical/ surgical history and allergies. Change in smoking/ alcohol/ family planning or vaccine status, and any changes to report in bone health/ cardiovascular risk were documented. If a patient showed willingness to consider change in behaviour, advice was given including signposting of resources to support behaviour change.
Conclusions: To date, this clinic has demonstrated proof of concept that patients with newly diagnosed AxSpA can be adequately managed via ANP-led care. Clinical supervision by the treating consultant remained in place for governance, including post review discussion where needed. Challenges remain to ensure review within agreed timeframes, but with only 7 of 257 appointments resulting in DNA, patients are happy to attend and receive evidence based nurse-led care that demonstrates value for money. Despite ANP-led care being under-utilised in AxSpA patients to date, this quality improvement initiative demonstrates a viable option to utilise nursing expertise effectively to create capacity for new patient appointments in consultant clinics.
| Scale | Visit 1 | Visit 2 | Visit 3 | MCID threshold |
|---|---|---|---|---|
| BASDAI | 4.53 | 3.55 | 3.50 | 10mm |
| BASFI | 3.71 | 2.72 | 2.80 | 7mm |
| BAS-G | 5.41 | 4.26 | 3.57 | 15mm |
| BASMI | 2.92 | 2.55 | 2.30 | 15mm |
Table 2.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of interest: EILEEN SHINNERS Pfizer, Novartis, Roche, Johnson&Johnson, Aine Gorman: None declared.