fetching data ... 
Background: Older adults with arthritis are at an increased risk of falls, due to factors such as joint pain and stiffness, muscle weakness, and poor balance [1-3]. The Otago Exercise Program (OEP) [4], implemented worldwide, reduces falls by 24% in high-risk populations [5]. While the OEP is cost-effective for older adults with arthritis [6], participation and adherence remain low [7].
Objectives: This study assessed whether training physiotherapists (PTs) in behaviour change techniques, combined with the use of a supporting digital tool, improved adherence to prescribed fall-prevention exercises among older adults with a history of falls.
Methods: This single-blind, parallel cluster randomised trial involved PTs working in the Greater Vancouver Area who had never received training in Brief Action Plaining. Individuals were randomly assigned (1:1) to receive the OEP training either alone ( OEP group ) or in combination with Brief Action Planning training and the use of an exercise tracking app ( OEP+ group ; ClinicalTrials.gov ID: NCT04851405). Brief Action Planning is a structured coaching approach involving goal setting, action planning, and monitoring with feedback. Randomisation was performed using numbers generated by SAS v9.4 in variable block sizes to ensure allocation concealment by a biostatistician not involved in the study. Following training, PTs were matched according to availability with older adults aged >70 years who had a Mini-Mental State Examination (MMSE) score >24/30 and a recent history of falls. Participants were recruited through the Vancouver Falls Prevention Clinic. PTs delivered the program through five home visits and three phone calls over a six-month period, followed by monthly phone calls for an additional six months. Older adults were instructed to complete individually tailored lower-body exercises (>3x/week) and undertake short walks (2x/week) for 12 months. OEP adherence (primary outcome) was self-reported by monthly calendars over 12 months. Secondary outcomes included Short Physical Performance Battery (SPPB, range 0-12; higher scores = better performance; minimum clinically important difference = 1.0;[8] scores ≤9 indicate higher risk of disability [9]), daily step count, and EuroQol-5D-5L assessed at baseline, 6 months, and 12 months. Exercise and walking adherence were calculated separately as: (sessions completed/total sessions expected) x 100. Falls were prospectively recorded on monthly calendars and defined as unintentional descent to the ground or a lower level, excluding events due to violent blows, loss of consciousness, stroke, or epileptic seizures. All participants were assessed at the Vancouver Fall Prevention Clinic between November 2021 to June 2025. Outcome assessors were blinded to the intervention allocation. Analyses followed an intention-to-treat approach using generalised linear models estimated via generalised estimating equations (GEE), adjusting for age and sex. Clustering of participants within PTs was accounted for by specifying PT as the clustering unit with robust sandwich standard errors. Fall counts were analyzed using quasi-Poisson regressions with robust sandwich standard errors to address potential overdispersion and clustering at the PT level. Sensitivity analyses included: 1) exclusion of outliers and 2) multiple imputation of missing data resulting from attrition or missed assessment visits.
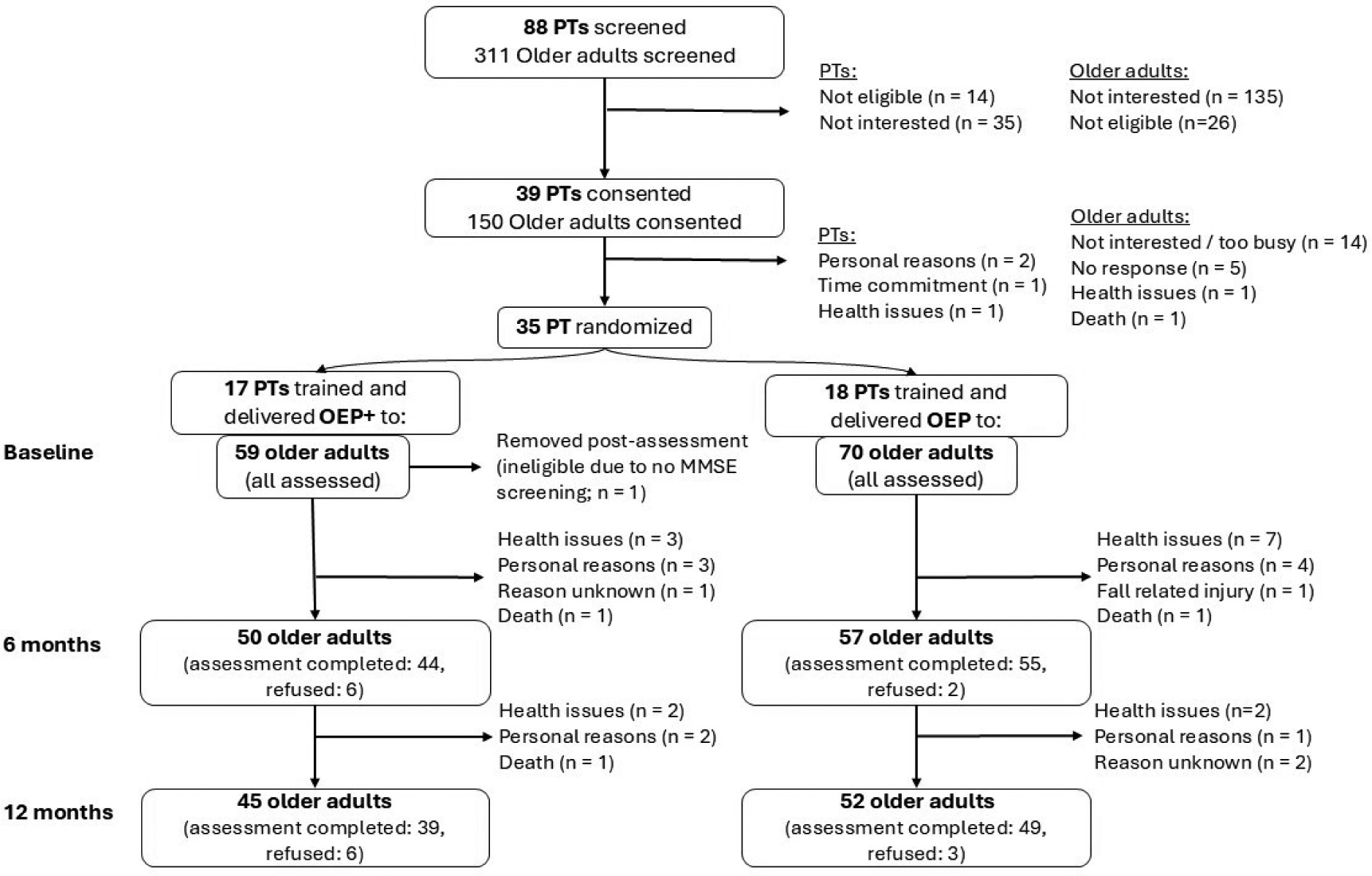
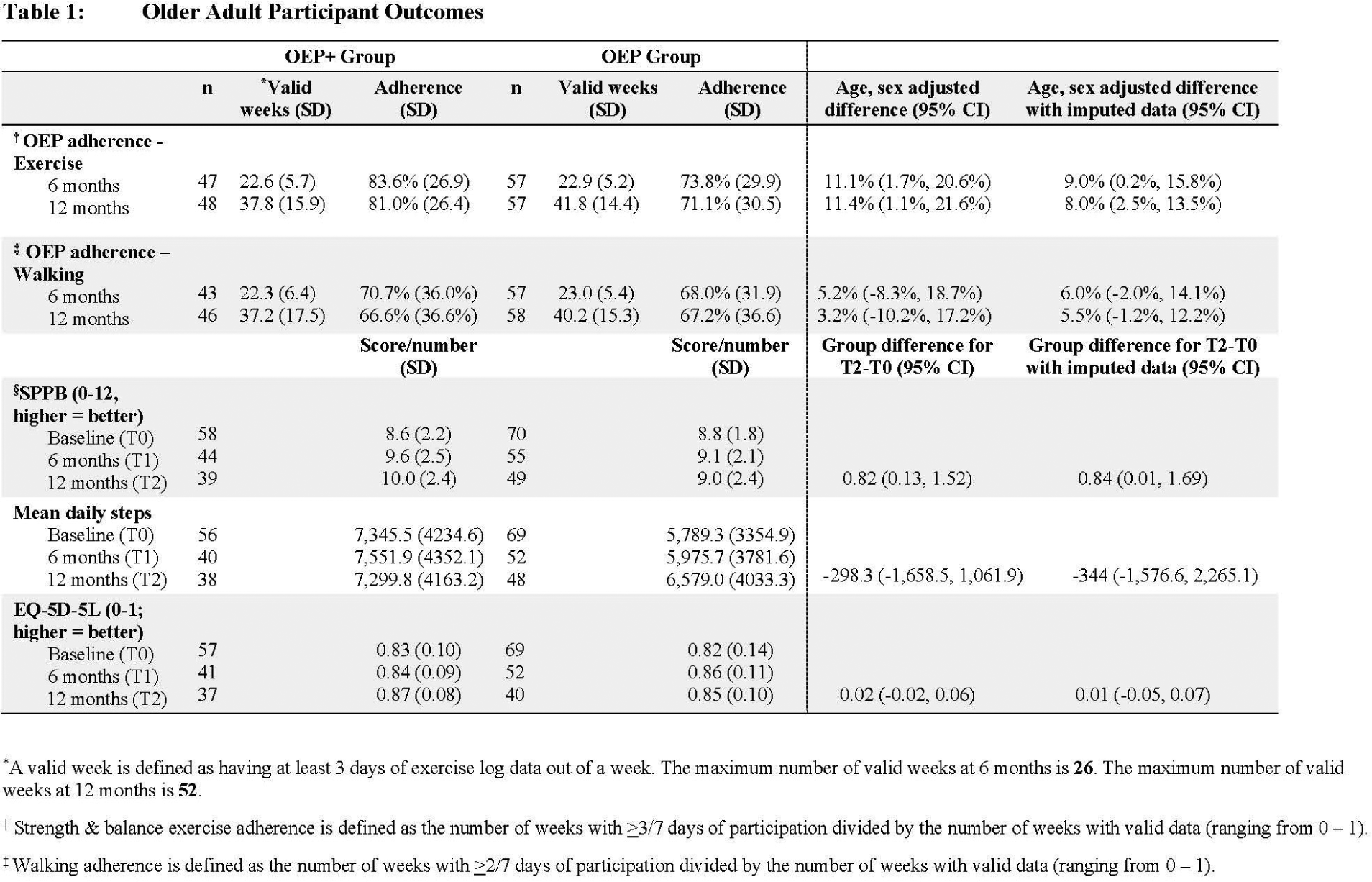
Results: Thirty-five PTs visited 128 older adults ( OEP+: 17 PTs, 94% female, years of practice: 14.4 (SD 10.0); 58 older adults, 81% female; OEP: 18 PTs, 89% female, years of practice: 11.7 (SD 10.1); 70 older adults, 69% female) ( Figure 1 ). Older adults in both groups were similar in age [OEP+: 80.9 years (SD 6.1); OEP: 82.0 years (SD 6.8)]. 61.7% reported arthritis, and 37.5% participated during the COVID-19 pandemic. The adjusted mean difference in lower-body exercise adherence at 12 months was 11.4% (95% CI, 1.1%, 21.6%), favouring OEP+ ( Table 1 ). Multiple imputation analyses showed a similar magnitude of difference in exercise adherence; 8.0% (95% CI, 2.5%, 13.5%). Walking adherence was similar between groups. Mean scores of SPPB were 10.0 (SD 2.4) for the OEP+ group and 9.0 (SD 2.4) for the OEP group. The adjusted mean difference from baseline to 12 months was 0.82 (95% CI, 0.13, 1.52). Over a mean follow-up of 318.2 (SD, 92.0) days, 78 falls occurred in the OEP+ group and 178 in the OEP group. The estimated fall rate per person-year was 2.71 and 4.26, respectively. The incidence ratio was 0.60 (0.27, 1.34), and the magnitude of result did not change after applying multiple imputation 0.62 (0.29, 1.37).
Conclusions: Otago Exercise Program, delivered by PTs trained in Brief Action Planning and supported by an exercise tracking app, was associated with greater exercise adherence and meaningfully improved physical function in older adults who had a history of falls. These results highlight the value of equipping PTs with behaviour change techniques and digital tools to strengthen the delivery and uptake of evidence-based fall prevention exercise programs for older adults.
Paticipant Flow Diagram
REFERENCES: [1] Wilfong JM, et al. Arthritis Care Res. 2023;75(11):2336–2344.
[2] Zhang Y, et al. Arthritis Res Ther. 2023;25(1):184.
[3] Guo X, et al. Semin Arthritis Rheum. 2023;60:152186.
[4] Campbell AJ, et al. BMJ. 1997;315(7115):1065–1069.
[5] Sherrington C, et al. Cochrane Database Syst Rev. 2019;1(1):Cd012424.
[6] Abdulrazaq S, et al. BMC Health Serv Res. 2018;18(1):574.
[7] Liu-Ambrose T, et al. J Am Geriatr Soc. 2008;56(10):1821–1830.
[8] Guralnik JM, et al. N Engl J Med. 1995;332(9):556–562.
[9] Gonçalves RS, et al. J Geriatr Phys Ther 2023;46(4):E127–E136.
Acknowledgments: NIL.
Disclosure of interest: None declared.