fetching data ... 
Background: Current B-cell-depleting strategies mainly target CD20 or CD19, including recent advances such as anti-CD19 CAR-T cell therapies in autoimmune diseases (AID) [1]. However, autoantibodies are produced by plasma cells, which do not express CD19 or CD20. Plasma cells and plasmablasts are known to express BCMA while its expression is very low or absent in other B cell subsets. Teclistamab, an anti-BCMA × anti-CD3 T-cell engager approved for multiple myeloma, has been successfully tested in a small number of AID patients, leading to prolonged drug-free remission.[2,3] Although teclistamab does not bind B cells in vitro 4 in healthy controls, clinical data report complete circulating B-cell depletion in both multiple myeloma 5 and AID [2]. In lupus, BCMA is upregulated on all circulating B-cell subsets compared to controls, but at levels too low to explain complete depletion [6]. BCMA also exists in a soluble form (sBCMA), which correlates with lupus disease activity and may represent an accessible biomarker of cell targets of anti- BCMA × anti-CD3 T-cell engagers.
Objectives: To evaluate sBCMA as a tissular plasma-cell biomarker in AID and to investigate the mechanisms underlying total B-cell depletion induced by teclistamab in AID patients compared to healthy controls.
Methods: Serum sBCMA levels were quantified using Meso Scale Discovery assays in 19 healthy controls (HC), 6 patients with systemic lupus erythematosus (SLE), 24 with Sjögren’s disease (SjD), and 35 with rheumatoid arthritis (RA) who had not received any B-cell-depleting therapy in the previous year. BCMA expression was assessed by immunohistochemistry in salivary gland biopsies from 13 SjD patients and sicca controls.
Peripheral blood mononuclear cells (PBMCs) from 9 RA, 10 SjD and 8 HC were isolated and cultured in vitro with either teclistamab (100 nM) or control medium for 48 hours. Flow cytometry was performed at baseline and after teclistamab treatment in vitro to characterize B-cell subsets and assess BCMA expression. One SjD patient was treated in vivo with teclistamab and monitored at baseline, 7 days and 1 month. Correlations were analyzed using Spearman’s correlation. Means were compared using a t-test for parametric data and the Mann–Whitney test for nonparametric data.
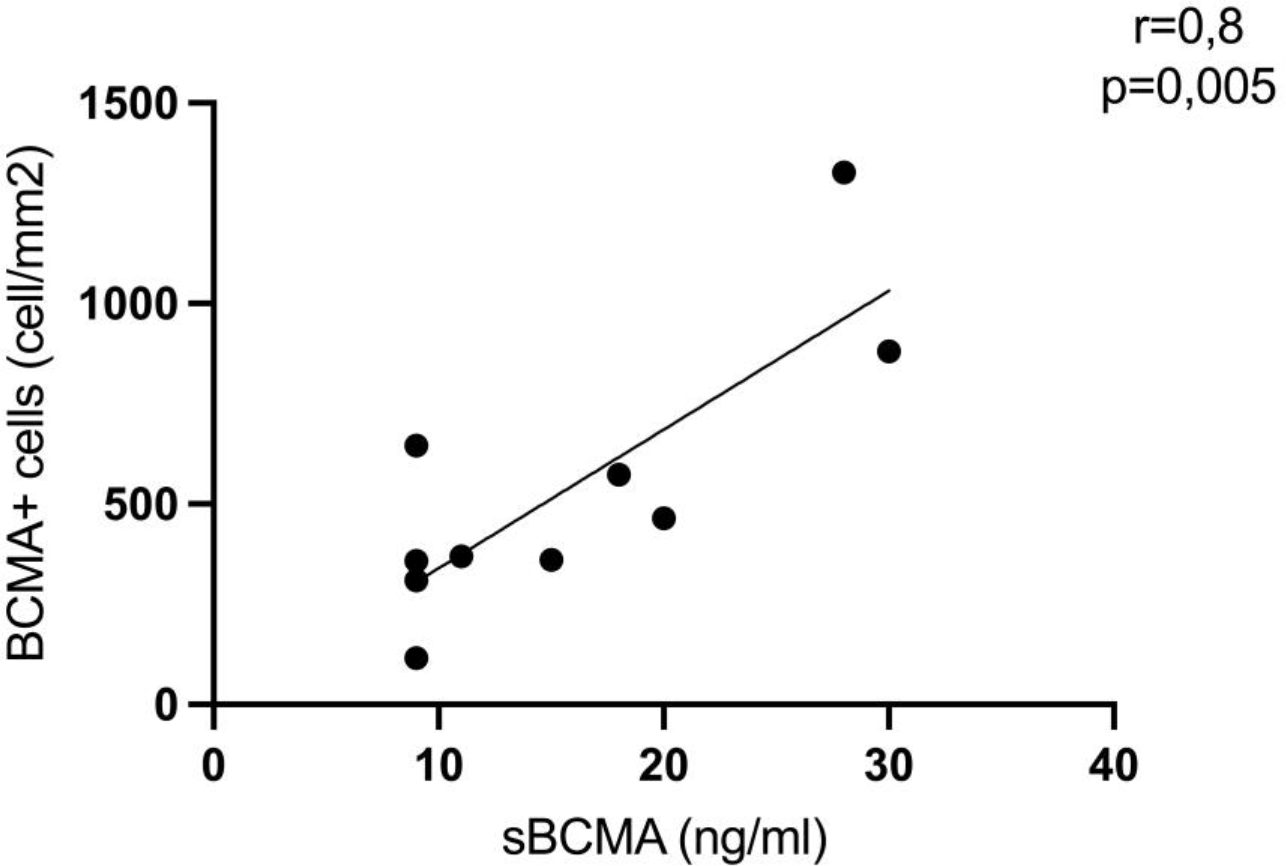
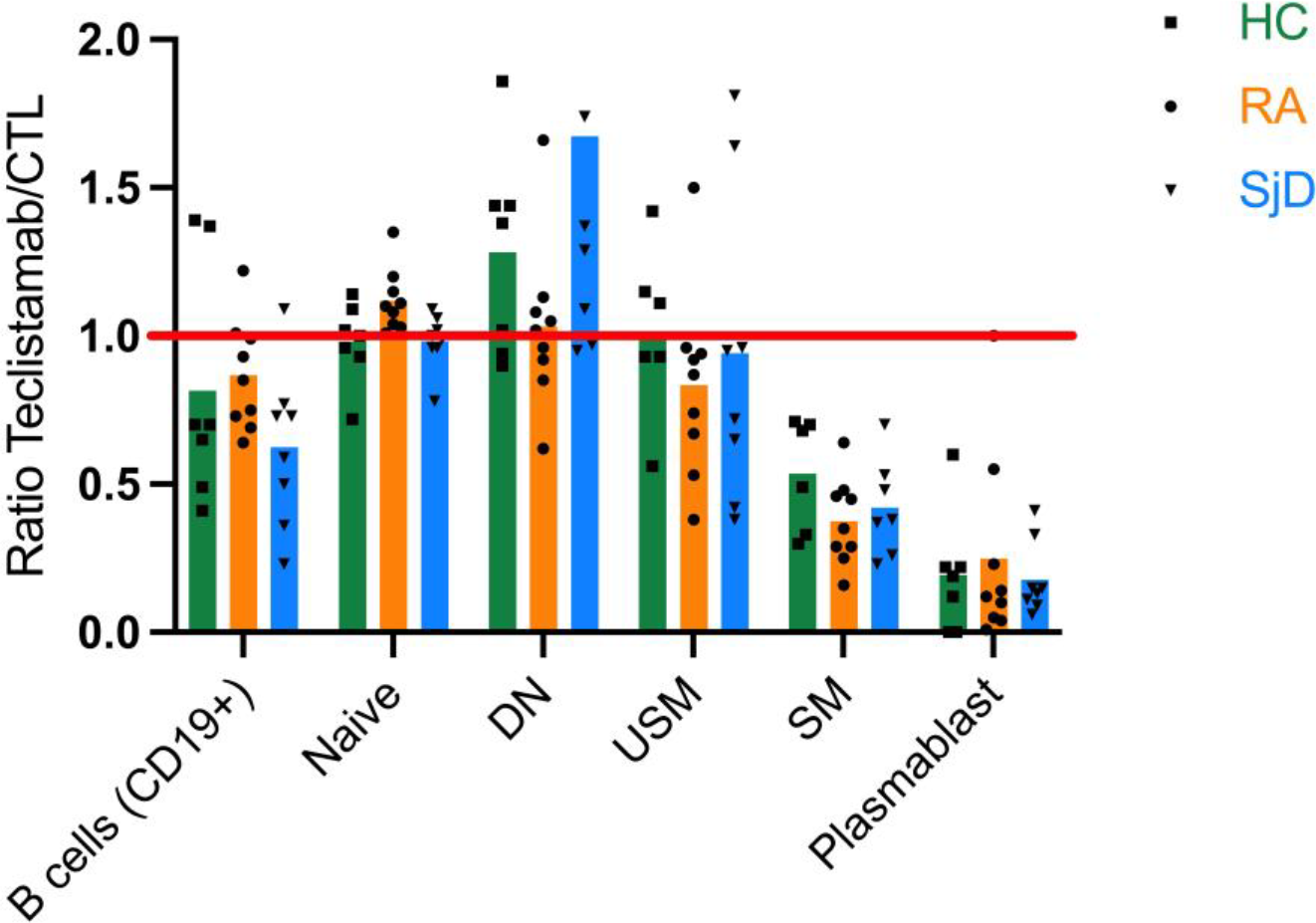
Results: sBCMA levels were increased in AID compared with HC (16.0 vs 12.5 ng/mL, p = 0.002) and correlated with disease activity in both RA and SjD. sBCMA strongly correlated with the number of BCMA-positive cells in salivary gland biopsies (Figure 1). In contrast, BCMA expression on circulating B cells did not correlate with sBCMA levels, confirming that sBCMA reflects the plasma-cell compartment rather than BCMA expression on peripheral B cells. BCMA expression was low on B cells from both AID patients and HC and was similar across B-cell subsets, except for plasmablasts. In vitro, 48 hours of teclistamab induced only partial B-cell depletion (23%). The mean depletion was more pronounced in switched memory B cells (57%) and plasmablasts (79%), with no significant differences between HC and AID patients (Figure 2). Correlations between global B-cell depletion and BCMA expression levels at baseline or disease activity were not significant. Similar results were observed in vivo seven days after teclistamab treatment in one SjD patient, with persistence of only naïve B cells, followed by complete B-cell depletion after one month.
Conclusions: Together, these data demonstrate that sBCMA is an accessible biomarker of tissue plasma-cell involvement in SjD and probably in other AID. Targeting BCMA with a T-cell engager may induce immune reset through preferential depletion of circulating memory B-cells and plasmablasts. The mechanism of this B-cell depletion does not rely only on the presence of BCMA at the membrane that is low and probably involves other mechanisms linked to T-cell activation.
Correlation between BCMA staining in salivary gland biopsies and serum sBCMA levels in SjD and sicca controls (Spearman correlation)
Effect of teclistamab on B-cell subsets: ratio of frequencies between teclistamab-treated and control medium–treated (CTL) cells after 48h. A ratio < 1 indicates a depletion of the subset following teclistamab treatment.
DN: double negative; USM: unswitched memory; SM: switched memory
REFERENCES: [1] Müller Fabian, Taubmann Jule, Bucci Laura, et al. CD19 CAR T-Cell Therapy in Autoimmune Disease — A Case Series with Follow-up. New England Journal of Medicine 2024; 390 : 687–700.
[2] Hagen M, Bucci L, Böltz S, et al. BCMA-Targeted T-Cell–Engager Therapy for Autoimmune Disease. New England Journal of Medicine 2024; 391 : 867–9.
[3] Alexander T, Krönke J, Cheng Q, Keller U, Krönke G. Teclistamab-Induced Remission in Refractory Systemic Lupus Erythematosus. New England Journal of Medicine 2024; 391 : 864–6.
[4] Pillarisetti K, Powers G, Luistro L, et al. Teclistamab is an active T cell-redirecting bispecific antibody against B-cell maturation antigen for multiple myeloma. Blood Adv 2020; 4 : 4538–49.
[5] Frerichs KA, Verkleij CPM, Mateos MV, et al. Teclistamab impairs humoral immunity in patients with heavily pretreated myeloma: importance of immunoglobulin supplementation. Blood Advances 2023; 8 : 194–206.
[6] Martin J, Cheng Q, Laurent SA, et al. B-Cell Maturation Antigen (BCMA) as a Biomarker and Potential Treatment Target in Systemic Lupus Erythematosus. Int J Mol Sci 2024; 25 : 10845.
Acknowledgments: NIL.
Disclosure of Interests: None declared.