fetching data ... 
Background: Childhood-onset Still disease (Systemic Juvenile Idiopathic Arthritis, SD), Kawasaki disease (KD), and Multisystem Inflammatory Syndrome in Children (MIS-C) are distinct pediatric inflammatory disorders that present with overlapping systemic manifestations including persistent fever, rash, mucocutaneous changes, elevated inflammatory markers, and, in many cases, multi-organ involvement. These overlaps create diagnostic uncertainty, underscoring the need for high-resolution biomarker profiling to identify disease-specific signatures – especially since early diagnosis is challenging and therapeutic approaches and complications differ substantially across conditions.
Objectives: Our goal was to identify soluble biomarkers capable of distinguishing MIS-C, KD, and SD at the time of presentation. In addition, we aimed to delineate shared versus disease-specific immune pathways.
Methods: Five groups were studied: Healthy Children (HC, 15 participants), Control Covid (CC, 18 participants), MIS-C (22 patients), SD (8 patients), and KD (15 pre-pandemic patients). CC serum was collected at a median of 3.7 weeks [3.1-4.7] after acute COVID infection, corresponding to the time frame of MIS-C onset in the MIS-C group. MIS-C, SD, and KD serum was collected at the time of admission prior to treatment. Serum was analysed using the Olink Target 96 Inflammation panel (
Results: The MIS-C group was balanced by gender (females 45.5%) with the median age of 7.5 years. KD patients had a median age of 2, with 33% female participants. SD
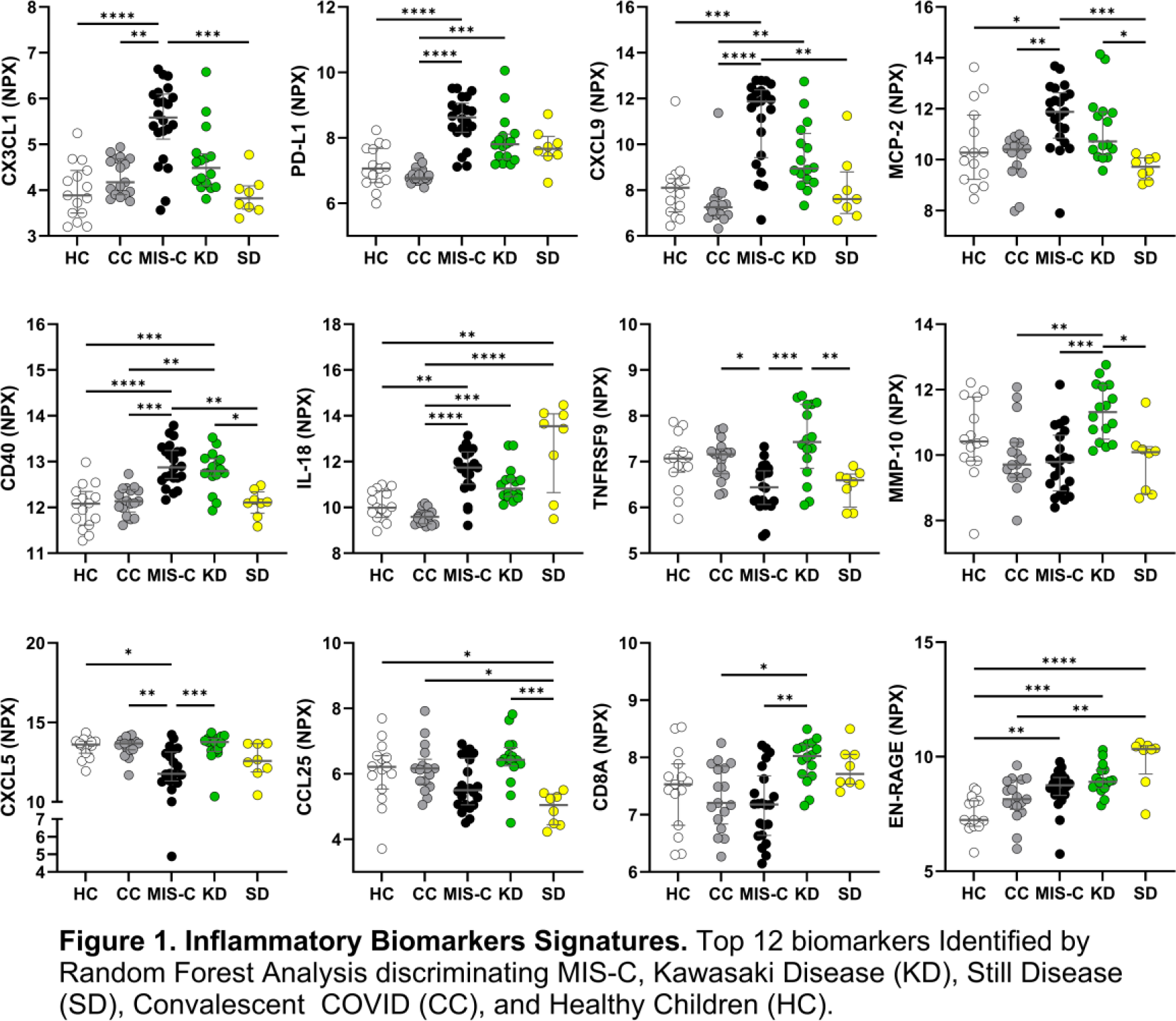
had a median age of 14 and included 37% female. CC had a median age of 7.5, with 45% female. HC had a median age of 5.6 years and included 40% females. Random forest analysis of the olink data identified eleven key cytokines and chemokines (CXCL1, PD-L1, CXCL9, MCP-2, CD40, IL-18, TNFRSF9, MMP-10, CXCL5, CCL25, CD8a, EN-RAGE/ S100A12) showing differential regulation across MIS-C, SD, and Kawasaki disease (Figure 1) and capable of classifying them (OOB estimate of error rate: 22.22%). Unsupervised clustering using this set of biomarkers identified two main clusters. The first cluster comprised cytokines that were markedly upregulated in MIS-C compared with both SD and Kawasaki disease, and with SD showing the lowest expression. These included CX3CL1, PD-L1, CXCL9, MCP-2, CD40, and IL-18. However, IL-18 had heterogeneous behavior in the SD group, with 5 out of 8 patients showing very high level of expression. The second cluster of biomarkers included cytokines that were mostly upregulated in Kawasaki patients. These included TNFRSF9, MMP10, CXCL5, CCL25, CD8a and EN-RAGE. Of note, in the SD group, EN-RAGE showed heterogeneous behavior with 5 patients showing high levels paralleling IL-18 upregulation. Consistent with the previous report, the SD group showed the lowest Interferon gamma signature, as measured by the levels of CXCL9, 10, and 11, with the exception of 1 patient (SD8) who, according to the clinical criteria, developed macrophage activation syndrome (MAS) and showed higher expression for these markers. Interestingly, this patient was misclassified inside the Kawasaki group. In general, all Kawasaki patients were classified together except for 2 (K12 and K13), which were grouped with the majority of MIS-C patients. Among the markers defining more specifically Kawasaki patients, we identified TNFRSF9 and MMP-10, the latter probably associated with coronary artery lesions as previously reported. Although the majority of MIS-C patients (15 out of 22) were classified together, 3 were classified inside the Kawasaki group and 4 within the SD group. In general, MIS-C patients showed the strongest interferon gamma-associated signature.
Conclusions: Serum proteomic profiling identified distinct inflammatory signatures differentiating MIS-C, Kawasaki disease, and SD, while also revealing partially shared immune pathways between MIS-C and SD.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Tetyana Pidkova: None declared, Victor Urrea: None declared, Rosa Pino: None declared, Marta Vidal: None declared, Ruth Aguilar: None declared, Gemma Moncunill: None declared, Carlota Dobano: None declared, Bonaventura Clotet: None declared, Jordi Antón Sobi, Novartis, Sobi, Novartis, Sobi, Novartis, Claudia Fortuny: None declared, Julià Blanco: None declared, Benjamin Trinité: None declared.