fetching data ... 
Background: Rheumatoid arthritis (RA) may accelerate age-related functional decline. However, evidence on how ageing affects both self-reported and performance-based physical function in older adults with RA – especially in direct comparison with population controls – is limited.
Objectives: To investigate the effect of age on five measures of physical function in older adults with RA compared to population controls.
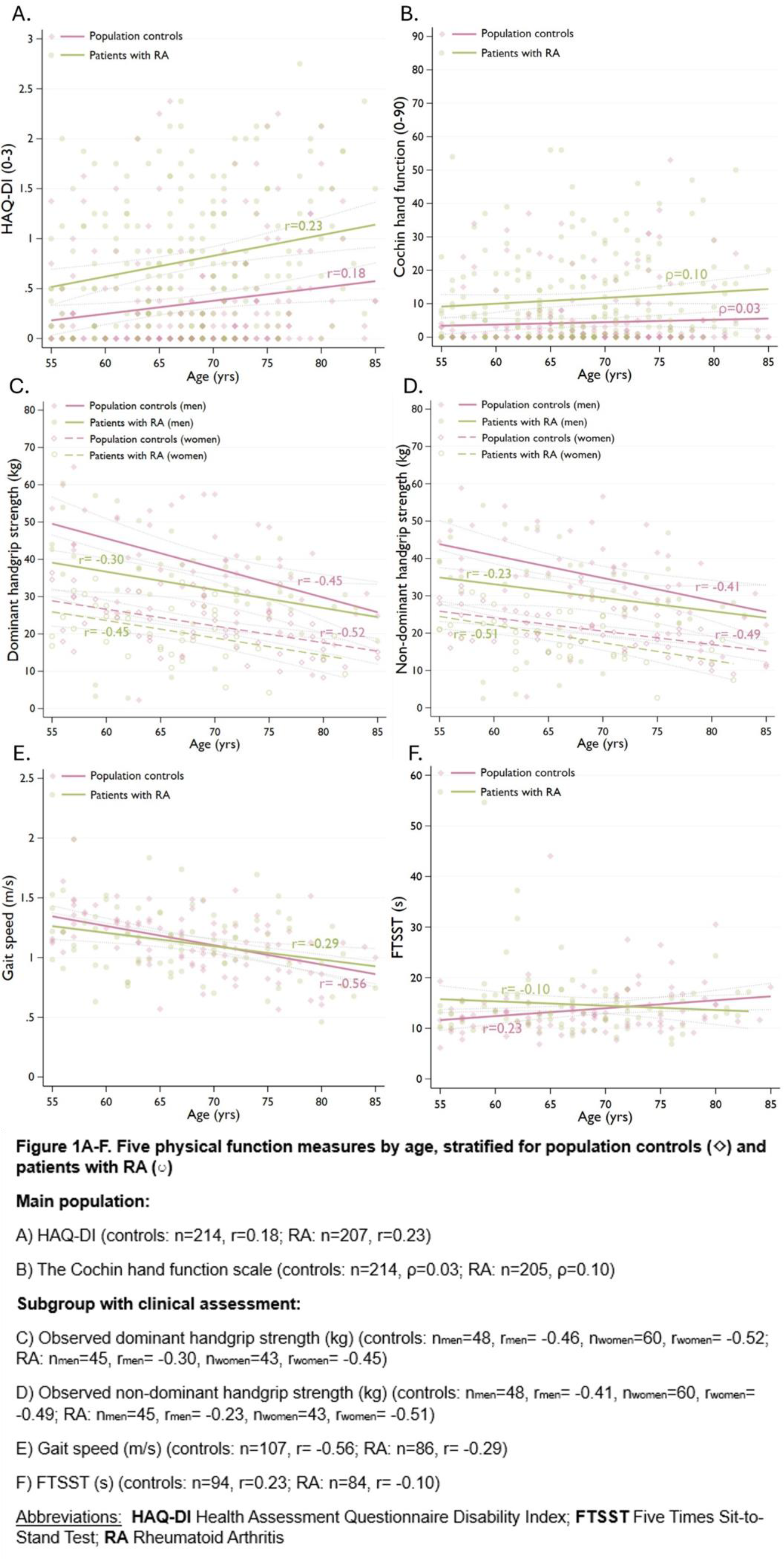
Methods: Cross-sectional data from the STudying Ageing in Rheumatoid arthritis (STAR) study was used including patients with RA and population controls without inflammatory rheumatic disease aged 55–85 years. Physical function was assessed using five measures: two self-reported questionnaires – the Health Assessment Questionnaire-Disability Index (HAQ-DI; 20 items; 0=no disability, 3=maximum disability) and the Cochin hand function scale (18 items; 0=no functional hand disability, 90=maximum disability) – and three performance-based tests available in a subgroup: Handgrip strength (HGS; kg) measured with a dynamometer, gait speed assessed by the four-meter walk test (m/s) and the Five-Times Sit-to-Stand Test (FTSST; s). Correlations between age and physical function were explored separately for RA patients and controls and visualized using scatter plots. Multivariable linear regressions assessed associations between age, group (RA/control) and physical function, adjusting for sociodemographic and clinical factors. Interactions age*group were tested. Cochin scores were analysed using zero-inflated negative binomial (ZINB) regression due to an excess of zeros. Sensitivity analyses included additional RA patients aged ≥70 years who could not complete the full protocol (only for HGS and gait speed). Additionally, multivariable logistic regressions assessed clinically relevant thresholds for impaired function (HAQ-DI: >1; Cochin: no thresholds available; HGS: gender- and BMI-specific Fried frailty criteria thresholds [1]; Gait speed: ≤0.8 m/s [2]; FTSST: >15.0 s [2]).
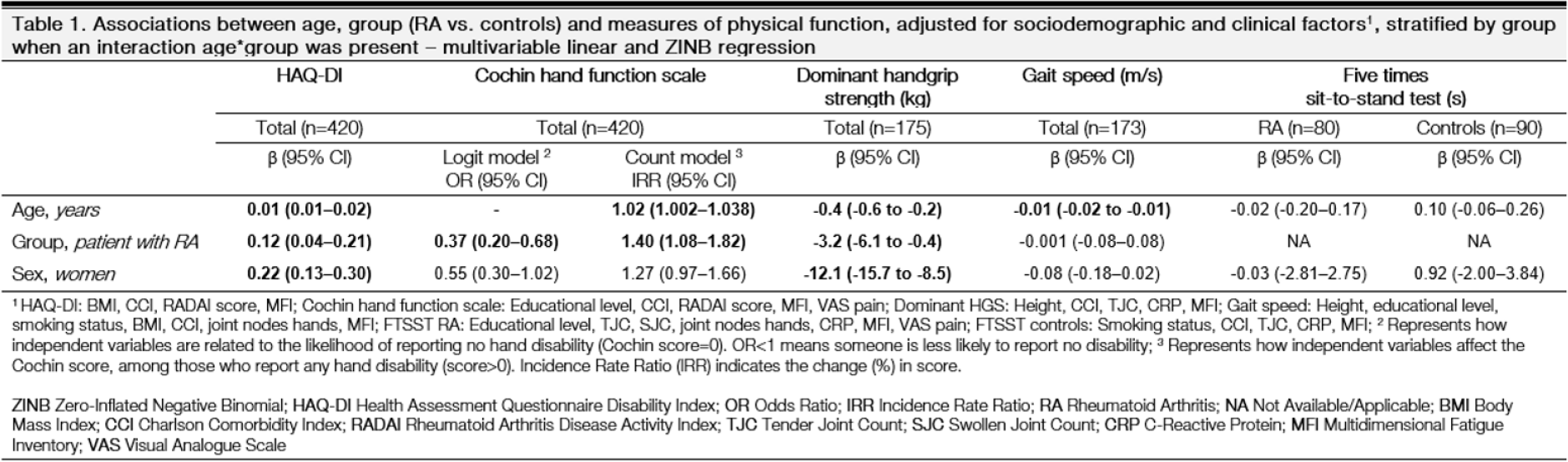
Results: A total of 421 participants were included: 207 patients with RA (mean age 68 (SD 7); 62% women) and 214 population controls (mean age 68 (7); 60% women). The subgroup with performance measures comprised 196 participants: 88 patients with RA (mean age 67 (8); 51% women) and 108 controls (mean age 69 (8); 56% women). The additional RA group aged ≥70 years for sensitivity analysis included 45 patients (mean age 77 (9); 53% women). Correlations with age were generally weak (range r RA =-0.10 to 0.29; r controls =-0.56 to 0.23), except for HGS (range r RA =-0.23 to -0.51; r controls =-0.41 to -0.52) (Figures 1A-F). No meaningful age*group interactions were observed, except for a small effect on the FTSST, where older age seemed to be associated with a longer FTSST time among controls (although not statistically significant; β age = 0.10, 95%CI: -0.06–0.26), while no association was present in patients with RA (β age = -0.02, 95%CI: -0.20–0.17) (Table 1). In multivariable linear regressions, each additional year of age was associated with worse HAQ-DI (β age =0.01, 95%CI: 0.01–0.02), a 2% worsening in Cochin hand disability (count model), lower handgrip strength (β age = -0.4 kg, 95%CI: -0.6 to -0.2), and slightly slower gait speed (β age = -0.01, 95%CI: -0.02 to -0.01) (Table 1). RA was independently associated with worse HAQ-DI (β RA =0.12, 95%CI: 0.04–0.21), 40% higher Cochin scores among those with hand disability, and lower handgrip strength (β RA = -3.2 kg, 95%CI: -6.1 to -0.4), but not with gait speed or FTSST (Table 1). Fatigue and pain were the main covariables attenuating age or group effects on physical function. In multivariable logistic regressions with the outcomes dichotomised, an age*group interaction was now found for Cochin hand function instead of FTSST (RA: OR age =1.07, 95% CI: 1.01–1.13; controls: OR age =1.00, 95% CI: 0.95–1.05). Comparable to linear regression, age increased the odds of mild to severe HAQ-DI, diminished handgrip strength (Fried criteria), and slow gait speed. Moreover, RA remained associated with HAQ-DI>1 and diminished handgrip strength. Including the additional RA group aged ≥70 years slightly strengthened group (RA vs control) effects, and age-gait speed correlations became slightly stronger (from r= -0.29 to r= -0.36).
Conclusions: Although RA is associated with a persistent functional disadvantage in older adult patients, the effect of age on the decline in functional ability was not different compared to the general population. The decline in physical function may rather reflect generic age-related than RA disease-specific processes, provided patients receive standard-of-care treatment. For older adults in general, an important opportunity to preserve overall function may therefore lie in addressing common geriatric syndromes (e.g. sarcopenia, frailty). However, for younger diagnosed patients, early and effective disease control with appropriate therapy may help to preserve long-term function. Future and particularly longitudinal research, including larger cohorts of older patients, is needed.
REFERENCES: [1] Fried, L. P., et al. (2001). Frailty in older adults: evidence for a phenotype. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences , 56 (3), M146-M157.
[2] Cruz-Jentoft AJ, et al. (2019). Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing , 48(1):16-31.
Acknowledgments: NIL.
Disclosure of Interests: Saskia Truijen: None declared, Annelies Boonen UCB, Eli Lilly, Novartis, Sandoz, Alfasigma, AbbVie, Celgene, Sofia Ramiro AbbVie, Alfasigma, Eli Lilly, MSD, Novartis, Pfizer, Takeda, UCB, AbbVie, Alfasigma, Eli Lilly, MSD, Novartis, Pfizer, Takeda, UCB, Marloes van Onna Novartis, Pfizer, Alfasigma, Pfizer, ReumaNederland.