fetching data ... 
Background: Rheumatoid arthritis (RA) is a chronic autoimmune condition marked by progressive damage to joints and periarticular tissues [1]. Frailty is a condition marked by reduced physiologic reserve, which independently increases the risk of hospitalization, serious infections, and death. Frailty and pre-frailty are more prevalent in individuals with RA versus the general population [2] and patients with RA tend to develop frailty at younger ages [3]. Despite this, frailty is not routinely incorporated into RA risk stratification or longitudinal care. How RA and its clinical features influence the development of frailty over time remains unclear.
Objectives: To assess the risk of incident frailty in RA versus non-RA and by decade of RA incidence/index and to identify key risk factors for incident frailty.
Methods: We conducted a retrospective cohort study of residents of Olmsted County in Minnesota with incident RA in 2000-2019 and non-RA comparators from the same underlying population to evaluate the incidence and risk of frailty. Patients with RA were matched 1:1 with their non-RA counterparts based on age, sex, and index date. The index date was defined as the earlier meeting of the 1987 and/or 2010 RA criteria. All were followed until death, last medical contact or 6/30/2025. Frailty was assessed using a validated claims-based frailty index with a deficit-accumulation model from administrative data during the 12-month baseline period. The index yields a continuous score from 0 (not frail) to 1 (frail) and has been validated as a predictor to adverse health outcomes in population-based studies [4]. Frailty was defined as an index of ≥ 0.20. Aalen-Johansen methods were used to estimate the cumulative incidence of frailty adjusted for the competing risk of death. Cox models were used to examine factors associated with frailty, adjusting for index year, age, sex, smoking and obesity.
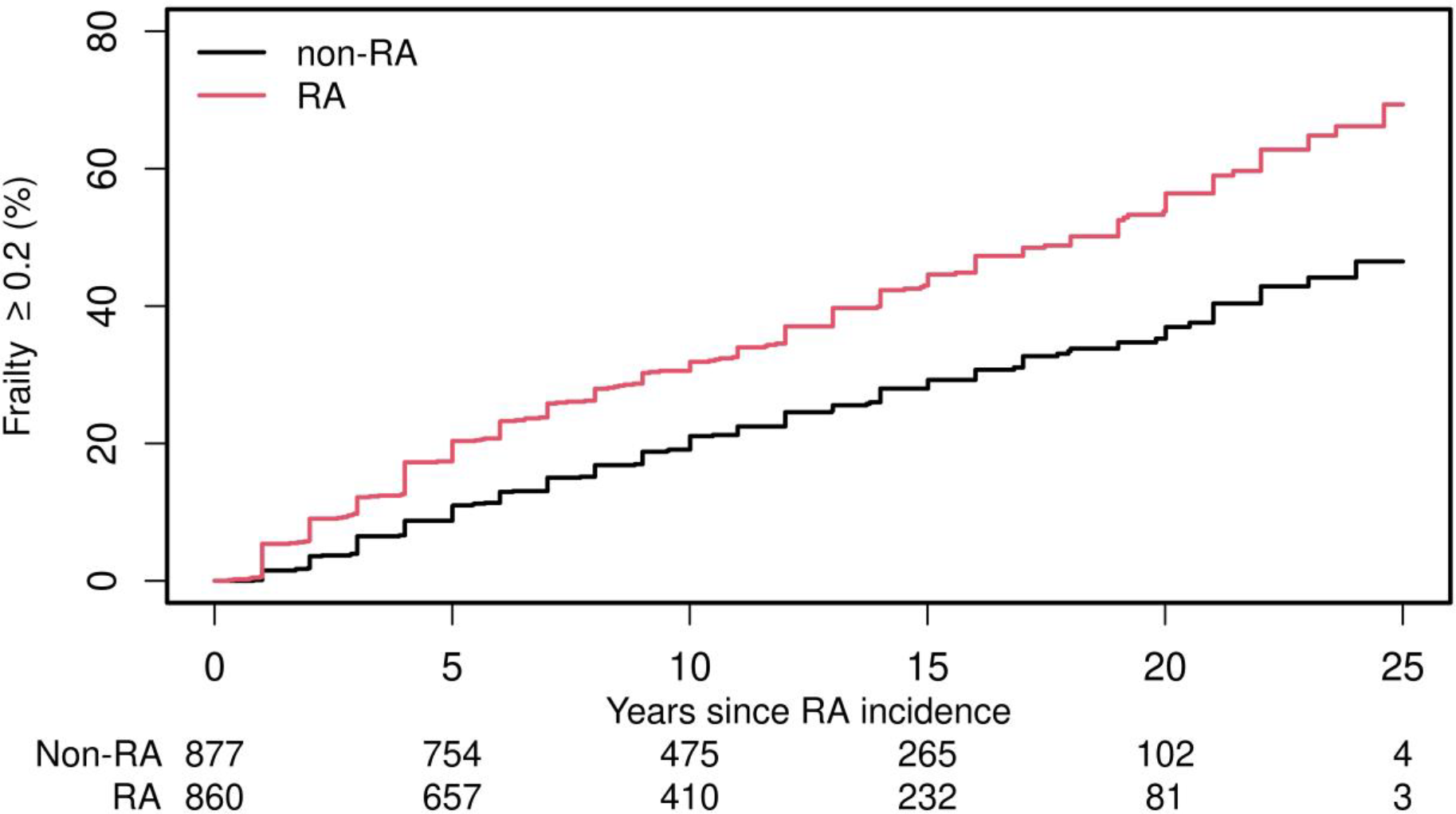
Results: The study included 910 individuals with RA and 910 matched non-RA individuals (mean age 55 years; 69.1% female in both cohorts). Fifty (5.5%) RA and 33 (3.6%) non-RA individuals met frailty criteria in the 1 year prior to index and were excluded from further analyses. The 10-year (30.6% [95% CI:27.5-34.0%] vs 19.1 [95% CI:16.6-22.1%] and 20-year (53.8% [95% CI:49.4-58.6%] vs 35.3% [95% CI:31.2-39.8%]) cumulative incidence of frailty was higher in individuals with RA than in non-RA (Figure 1). RA was associated with increased risk of frailty in the overall cohort (HR 2000-2019: 1.76,95% CI 1.49-2.08) and in each decade of RA incidence/ index (HR 2000-2009: 1.43,95% CI 1.16-1.77; HR 2010-2019: 2.38, 95%CI 1.81-3.12). More recent decade of index (2010-2019 versus 2000-2009) was associated with heightened risk of incident frailty in individuals with RA (HR 1.50, 95%CI 1.19-1.89), but not in those without RA (HR 0.76, 95% CI 0.57-1.02). This increased risk of frailty in individuals with incident RA in 2010-2019 compared to RA in 2000-2009 was mainly in those with RF/CCP-Antibody positive RA (HR 1.62, 95%CI 1.20-2.19), while not achieving statistical significance in seronegative RA (HR 1.31, 95%CI 0.90-1.88). Within the RA cohort, increasing age (HR 1.95 per 10 years, 95%CI 1.79-2.13) and more recent index year (HR 1.25, 95%CI 1.12-1.39) was associated with increased risk of incident frailty, while education was associated with reduced risk (HR 0.72 95%CI 0.57-0.89). Other risk factors for incident frailty in RA included former smoking (HR 1.49, 95%CI 1.18-1.88), current smoking (HR 2.22, 95%CI 1.67-2.95), obesity (HR 1.53, 95%CI 1.25-1.89), diagnosis of hypertension (HR 1.65, 95%CI 1.31-2.07), type 2 diabetes mellitus (HR 1.41, 95%CI 1.05-1.89) and dyslipidemia (HR 1.31, 95%CI 1.05-1.63) at incidence, as well as Charlson Comorbidity index (HR 1.56, 95%CI 1.38-1.77). RA disease characteristics that occurred prior to or within 1 year following RA incidence also increased risk of incident frailty: rheumatoid nodules (HR 1.52, 95%CI 1.09-2.12), severe extra-articular manifestations (HR 1.70, 95%CI 1.71-2.47), erythrocyte sedimentation rate per 5 unit increase at incidence (HR 1.03 (1.00-1.05), time-dependent exposure to biologics (HR 1.69, 95%CI 1.22-2.33), glucocorticoids (HR 1.69, 95%CI 1.14-2.52) and other DMARDs (HR 1.41, 95%CI 1.04-1.93) were also associated with increased frailty risk. In contrast, sex, race, RF and/or CCP seropositivity, large joint swelling, radiographic erosions/destructive changes, use of methotrexate or hydroxychloroquine were not associated with frailty.
Conclusions: Individuals with incident RA (2000-2019) have 1.8-fold higher risk of incident frailty compared to their non-RA counterparts. The excess frailty risk was greatest in the more recent RA incidence cohort, particularly among RF/CCP-positive patients. The risk is driven by older age, comorbidity burden, modifiable cardiovascular risk factors, and markers of more severe RA. Together, these findings show that frailty has become an increasingly important outcome in contemporary RA and stress the need for early identification and targeted risk-factor modification.
Cumulative incidence adjusted for competing risk of death.
REFERENCES: [1] Di Matteo, A., J.M. Bathon, and P. Emery, Rheumatoid arthritis. Lancet, 2023. 402(10416):p. 2019-2033.
[2] Salaffi, F., et al., Prevalence of frailty and its associated factors in patients with rheumatoid arthritis: a cross-sectional analysis. Clin Rheumatol,2019. 38(7) p.1823-1830. [3] Andrews,J.S.,et al., Frailty and reduced physical function go hand in hand in adults with rheumatoid arthritis: a US observational cohort study. Clin Rheumatol,2017.36(5):p. 1031-1039.
[4] Singh,N.,et al., Frailty and Risk of Serious Infections in Patients With Rheumatoid Arthritis Treated With Biologic or Targeted-Synthetic Disease-Modifying Antirheumatic Drugs. Arthritis Care Res (Hoboken),2024.76(5) p.627-635.
Acknowledgments: NIL.
Disclosure of Interests: None declared.