fetching data ... 
Background: Patients with iRMD are at increased risk for herpes zoster (HZ), especially in older patients and those on immunosuppressive medications. While the recombinant zoster vaccine (RZV) has proven effective in reducing the risk of HZ by inducing CD4 T-cell responses in healthy individuals, data on immunogenicity in iRMD patients are scarce.
Objectives: This study aimed to evaluate cellular and humoral immune responses to RZV in iRMD patients stratified by age, and to identify factors associated with reduced immunogenicity. This interim analysis reports results of cellular immunogenicity over 12 months.
Methods: This prospective longitudinal study included patients with rheumatoid arthritis (RA), axial spondyloarthritis (axSpA), both <50 and ≥ 50 years of age, and giant cell arteritis (GCA), only in patients ≥ 50 years of age, who had received at least one RZV dose. Patients and disease characteristics were assessed including medication with csDMARDs, bDMARDs, tsDMARDs or glucocorticoids. Cell-mediated immunity (CMI) was measured through CD4+ glycoprotein E (gE)-specific T-cell activation before first dose visit (FDV) and 3-, 6- and 12-months post FDV (m3, m6 and m12 visits). Comparisons between timepoints were calculated by t-tests. CMI was analyzed separately for axSpA, RA and GCA using a mixed effects linear model with time as independent variable and patient-specific random intercept. The models were applied both with and without adjustment for age, sex and patient global of disease activity (PGA).
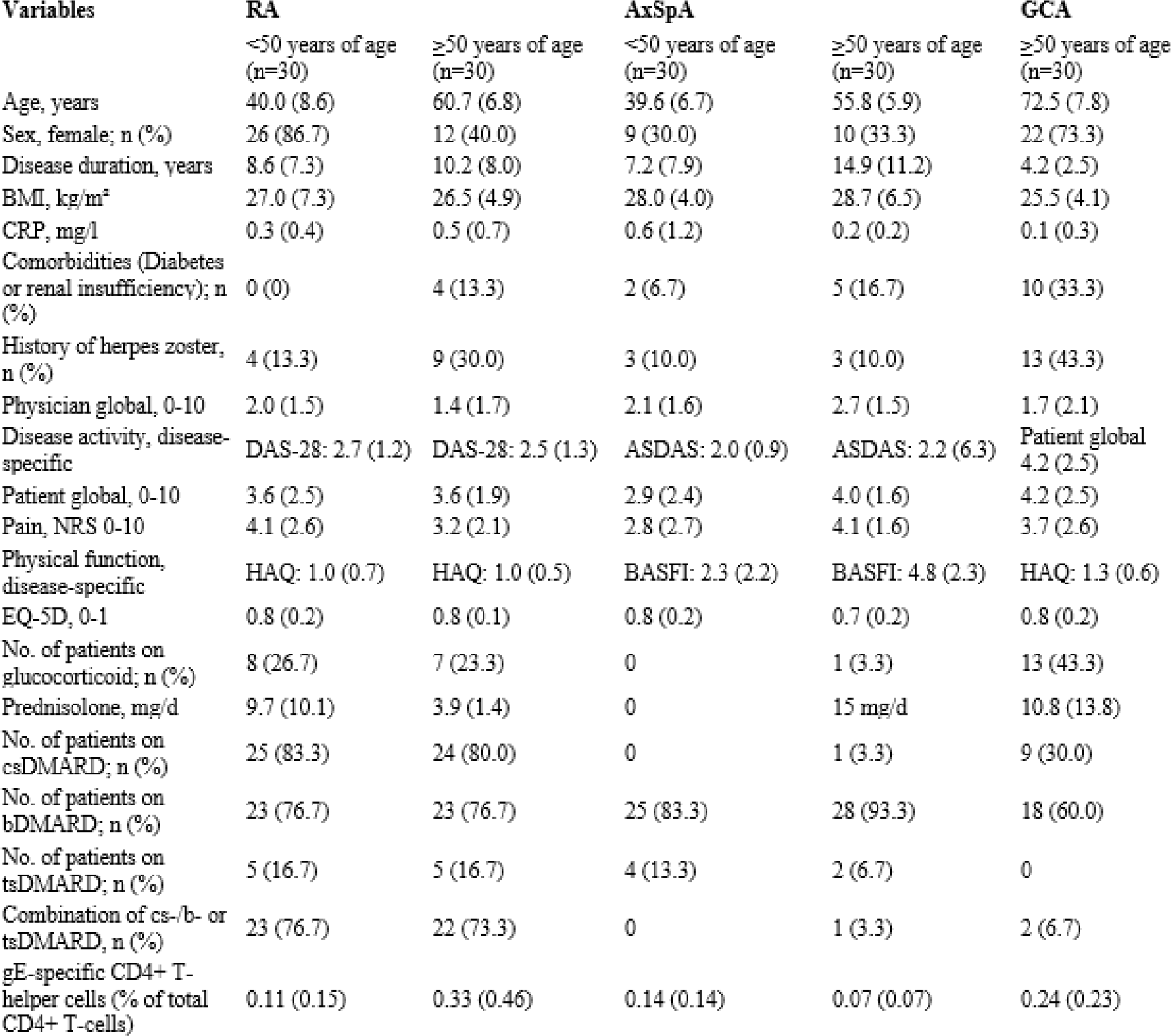
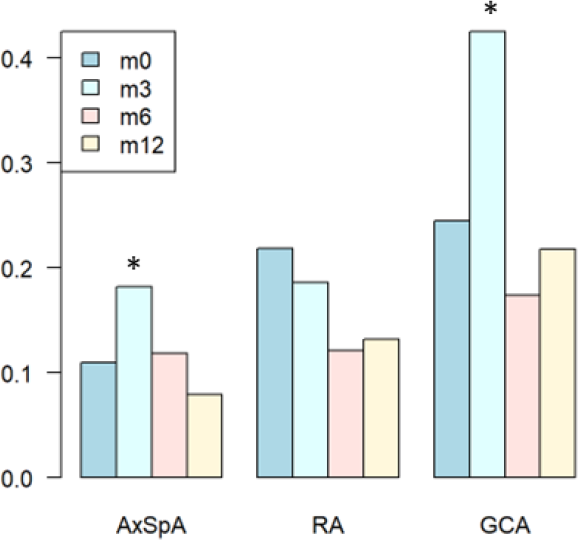
Results: 150 patients (60 RA, 30 <50 and 30 ≥ 50 years of age; 60 axSpA, 30 <50 and 30 ≥ 50 years of age, and 30 GCA, all ≥ 50 years of age) were enrolled of whom 145 (96.7%) patients received two RZV doses 2.2 (0.3) months apart (table 1). 32 patients (21.3%) had a history of past HZ, while 59 (39.3%), 117 (78%) and 16 (10.7%) patients received cs-, b- or tsDMARD, respectively, 98 of whom (65.3%) applied as monotherapy. Most patients (n=133) completed 12 months post FDV (88.9%). Baseline values were comparable between disease- and age-groups except for disease duration and history of HZ which were higher in older patients. All but one patient showed cellular immunity against VZV at baseline. The fraction of gE-specific T-cells peaked at month 3, but 35 of 135 patients (25.6%) with CMI results did not show an increase in CMI after vaccination. Both axSpA and GCA showed a significant increase in CMI at month 3, whereas no significant increase in CMI was observed at any other time points, nor in RA patients at month 3 (figure 1). On average, CMI values were twice as high in GCA patients as those in axSpA patients at all time points. A decline in CMI was observed over the entire study period in patients with axSpA (monthly change rate -0.008 (95%CI -0.012- -0.003)) and RA (-0.008 (95%CI -0.013- -0.003)) which was not the case in GCA ((-0.001 (95%CI -0.007- 0.004)). The findings were robust against adjustments with age as a significant predictor of a lower change rate.
Conclusions: Cellular immune responses to RZV peaked at month 3 in axSpA and GCA patients with a gradual decrease of CMI thereafter. However, about one quarter of patients did not show an increase in cellular immunity at all. Data on humoral immunogenicity are in progress to contextualize the immune response to RZV in these patient populations.
Table 1. Patients and disease characteristics at baseline stratified by age groups.
Frequencies of gE-specific CD4+ T-helper cells in iRMD patients over 12 months, stratified by disease
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.