fetching data ... 
Background: Antiphospholipid syndrome (APS) is a thrombo-inflammatory disease propelled by circulating autoantibodies, classified according to the 2023 ACR/EULAR criteria which integrate clinical and laboratory domains to better define the syndrome spectrum [1]. While platelets are central effector cells in thrombosis, their specific immunoregulatory roles in APS pathogenesis remain poorly understood. Beyond their classical haemostatic functions, platelets are increasingly recognized as active modulators of innate and adaptive immunity, capable of responding to pathogens and sterile inflammation through pattern recognition receptors and interactions with immune cells [2]. In APS, antiphospholipid antibodies not only drive a pro-thrombotic phenotype—including through mTORC2/Akt-mediated platelet activation [3]—but also engage platelet immune functions, potentially amplifying the inflammatory cascade via complement activation and neutrophil extracellular trap (NET) formation [4,5]. However, a systematic understanding of how platelet biology integrates these dual roles in APS is missing. Despite transcriptomic insights into other immune compartments—such as interferon signatures in leukocytes [6]—a comprehensive analysis of the platelet transcriptome, which could reveal disease-specific immuno-thrombotic pathways and biomarkers, is currently lacking.
Objectives: To delineate the platelet transcriptional landscape in APS, identify key immune-thrombotic pathways, and evaluate platelet-derived mRNA signatures as candidate diagnostic biomarkers.
Methods: We performed RNA sequencing on platelets isolated from 43 APS patients, 20 asymptomatic antiphospholipid antibody (aPL) carriers, and 20 healthy controls. Differential expression analysis, Gene Set Enrichment Analysis (GSEA), and Weighted Gene Co-expression Network Analysis (WGCNA) were used to identify dysregulated genes and pathways. Machine learning algorithms (LASSO, Random Forest, and SVM-RFE) were employed to identify diagnostic biomarkers. Pathway-gene complex networks were constructed to elucidate molecular interactions.
Results: Platelets in APS exhibit a unique transcriptomic signature marked not only by activation features but also by significant immune dysregulation, including upregulated Toll-like receptor pathways. Machine learning identified 15 key genes (DOCK5, FCER1G, HSP90AA1, etc.) with strong diagnostic potential (AUC 0.901–0.948). Additionally, functional enrichment analysis and WGCNA confirmed that high-titer, triple-positive aPLs (especially aβ2GPI) robustly activate coagulation and immune pathways, substantiating the “antibody-educated platelet” theory. Moreover, WGCNA revealed divergent molecular signatures for arterial versus venous thrombosis involving differences in aerobic electron transport, lipid metabolism, and small GTPase-mediated signaling.
Conclusions: This study provides a comprehensive transcriptomic framework of platelets in APS, uncovering novel biomarkers and pathways that link thrombosis and immune dysregulation. By integrating machine learning and network-based analyses, we enhance diagnostic precision and uncover mechanistic insights that may guide future precision medicine approaches in APS.
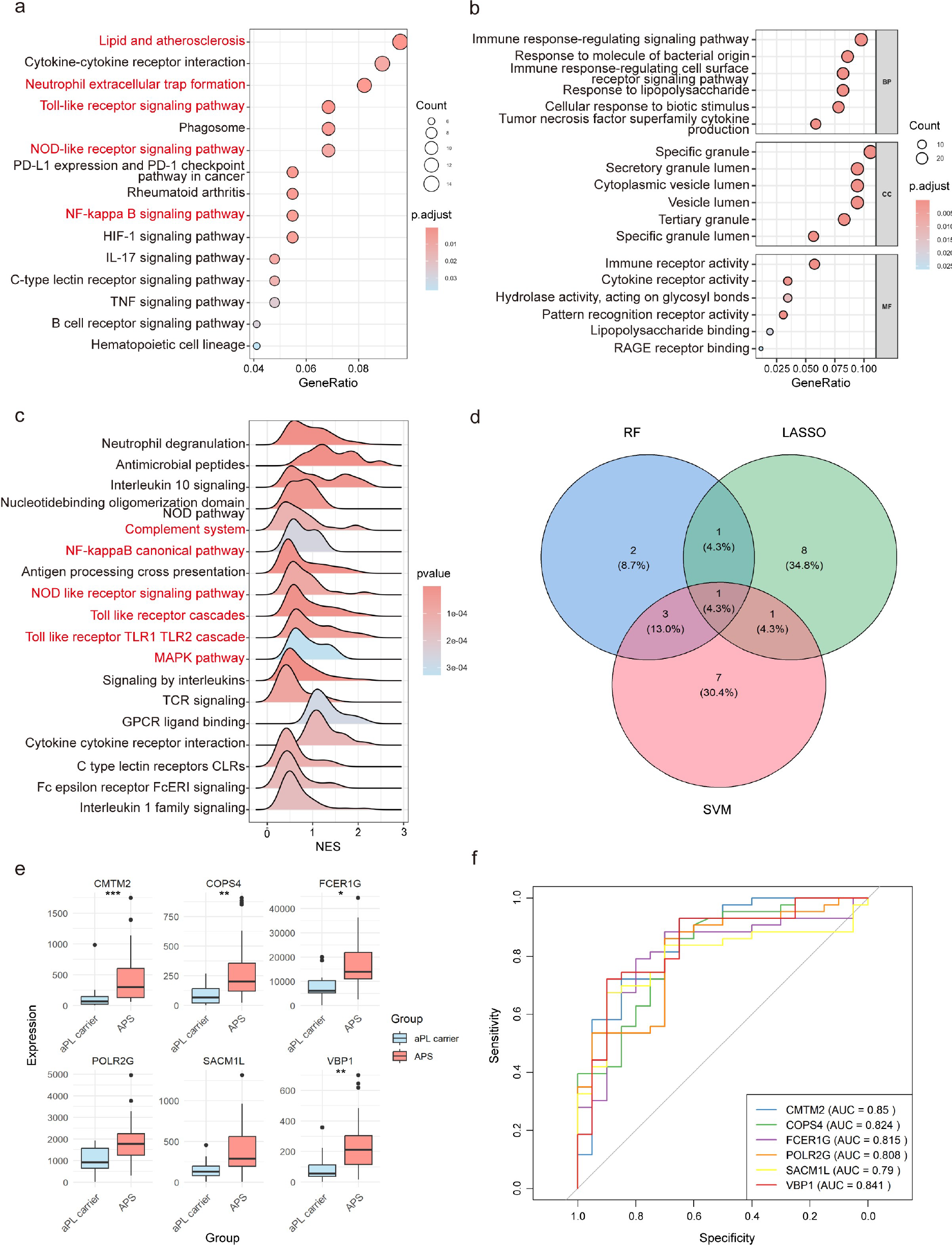
Platelet Transcriptomic Signature in APS Versus aPL Carriers: Enhanced Toll-Like Receptor Signaling in APS. (a) Dot plot showing KEGG analysis between APS patients versus aPL carriers. (b) Dot plot showing GO analysis between APS patients versus aPL carriers. (c) Ridge plot showing the GSEA of canonical pathways between APS patients versus aPL carriers. (d) Venn plot shows the number and percent of key genes screened by at least two machine learning methods. (e) Boxplot of key discriminative gene expression in APS patients and aPL carriers. (f) ROC curves and AUC rate of the feature genes. APS, antiphospholipid syndrome; aPL, antiphospholipid antibodies; KEGG, Kyoto Encyclopedia of Genes and Genomes; GO, gene ontology; GSEA, gene set enrichment analysis.
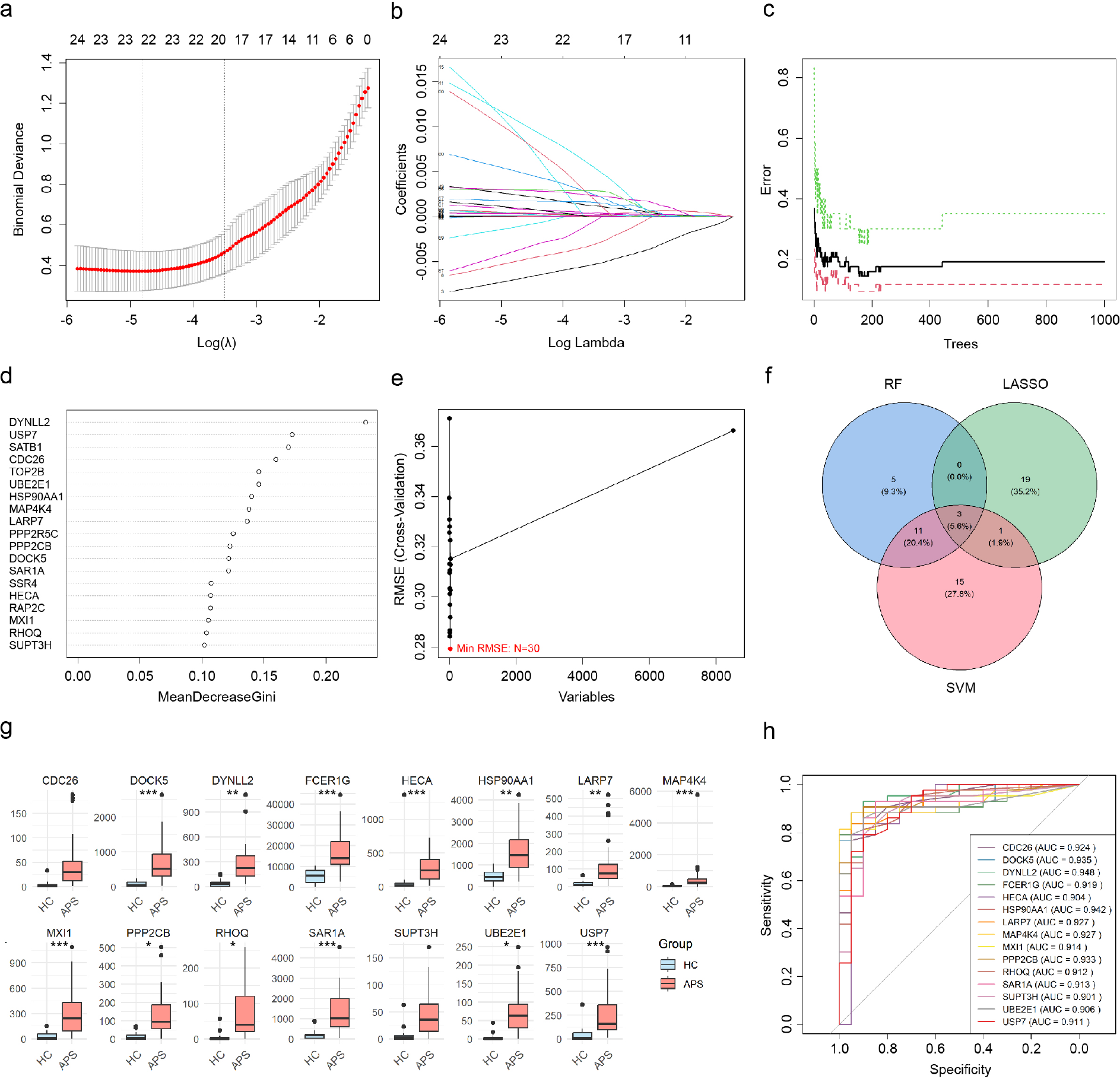
Machine Learning Identifies Key Discriminative Genes in APS Versus Healthy Controls: Robust Biomarkers for APS Diagnosis. (a, b) The performance in of 10-fold cross verification for tuning parameter in selection LASSO. (c) RandomForest error rate versus the number of classification trees. (d) Top 30 relatively important genes selected by randomForest. (e) Recursive feature elimination (SVM–RFE) algorithm selection. (f) Venn plot shows the number and percent of key genes screened by at least two machine learning methods. (g) Boxplot of key discriminative gene expression in APS patients and HC. (H) ROC curves and AUC rate of the feature genes.
REFERENCES: [1] Barbhaiya M, Zuily S, Naden R, et al. 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheum Dis 2023;82:1258–70.
[2] Koupenova M, Corkrey HA, Vitseva O, et al. The role of platelets in mediating a response to human influenza infection. Nat Commun 2019;10:1780.
[3] Tang Z, Shi H, Chen C, et al. Activation of Platelet mTORC2/Akt Pathway by Anti-β2GP1 Antibody Promotes Thrombosis in Antiphospholipid Syndrome. Arterioscler Thromb Vasc Biol 2023;43:1818–32.
[4] Peerschke EI, Yin W, Alpert DR, et al. Serum complement activation on heterologous platelets is associated with arterial thrombosis in patients with systemic lupus erythematosus and antiphospholipid antibodies. Lupus 2009;18:530–8.
[5] Tambralli A, Gockman K, Knight JS. NETs in APS: Current Knowledge and Future Perspectives. Curr Rheumatol Rep 2020;22:67.
[6] Cecchi I, Radin M, Barinotti A, et al. Type I interferon pathway activation across the antiphospholipid syndrome spectrum: associations with disease subsets and systemic antiphospholipid syndrome presentation. Front Immunol 2024;15:1351446.
Acknowledgments: NIL.
Disclosure of Interests: None declared.