fetching data ... 
Background: Pulmonary arterial hypertension (PAH) affects 8–12% of systemic sclerosis (SSc) patients, representing a life-threatening manifestation with 3-year mortality rates up to 48%. Why only a subset of patients with SSc presents PAH remains poorly understood, and earlier identification of individuals at increased risk is still an unmet clinical need.
Objectives: The objective of this study was to characterize the genetic component of SSc-PAH patients through a genome-wide association study (GWAS) aiming to enhance the understanding of the disease pathology and identify potential genetic markers related to disease progression.
Methods: We analyzed genomic data comprising 6,878 patients (999 SSc-PAH + and 5,879 SSc-PAH - ) and 16,630 healthy controls from the largest genomic scan in the disease in European-descent population [1]. SSc-PAH + cases were confirmed by right heart catheterization. Logistic regression adjusted for sex and the first five principal components were performed to seek associations to SSc-PAH: (1) SSc-PAH + vs healthy controls (2) SSc-PAH + vs SSc-PAH - . Variants were considered specifically associated with SSc-PAH if they reached genome-wide significance (p < 5E-8) and did not reach the suggestive significance threshold (p < 1E-5) in the SSc-PAH - vs healthy controls comparison. Functional annotation was performed using FUMA and ForgeDB.
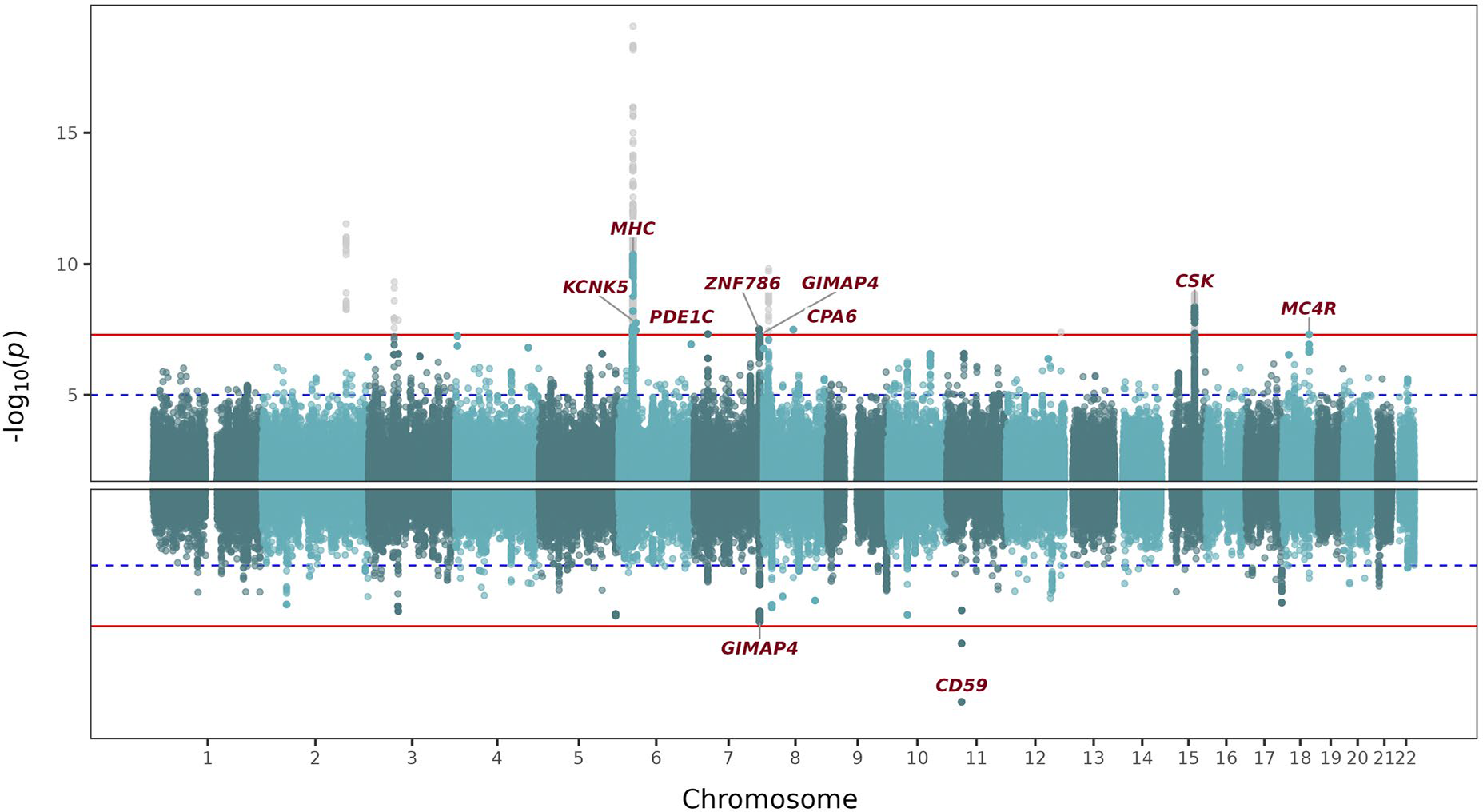
Results: 7 non-HLA genetic regions were identified when comparing SSc-PAH + vs healthy controls, such as those annotated to KCNK5 (rs111552071, p = 1.77E-8, OR = 2.05). KCNK5 encodes a potassium channel that might be involved in membrane potential changes. Interestingly, channelopathies have been linked to idiopathic PAH, particularly through K + channels regulating pulmonary artery smooth muscle cells. The other interesting finding is the association of variants located within the GIMAP family region, almost reaching the genome-wide significance (rs6960073, p = 5.13E-8, OR = 0.74) as also found in the SSc-PAH + vs SSc-PAH - comparison (rs11762140, p = 7.4E-8, OR = 0.74). Specifically, GIMAP4 is involved in T-cell apoptosis and could contribute to SSc-PAH pathogenesis via dysregulated immunity. Notably, these variants have been correlated with GIMAP4 altered gene expression in immune, lung and vascular tissues. Remarkably, when comparing SSc-PAH + vs SSc-PAH - , we identified one association annotated to CD59 (rs191009425, p = 6.45E-11, OR = 5.06), which encodes a complement regulatory protein that inhibits formation of the membrane attack complex. Its dysregulation may contribute to complement-mediated vascular endothelial injury in the pathogenesis of SSc-PAH.
Conclusions: The first GWAS of SSc-PAH revealed novel genetic loci that may contribute to the development of PAH in SSc patients. These findings could facilitate early identification of SSc patients at risk of developing PAH, enabling personalized monitoring strategies and timely interventions.
Miami plot showing SSc-PAH + vs healthy controls (top) and SSc-PAH + vs SSc-PAH - (bottom) comparisons. Chromosomes are displayed along the x-axis, and statistical significance is represented on the y-axis as –log10(p-value). The red line indicates the genome-wide significance threshold (p = 5E-8), while the blue dashed line marks the suggestive threshold (p = 1E-5). Variants in gray are significant but do not meet predefined specificity criteria for SSc-PAH.
REFERENCES: [1] López-Isac E, Acosta-Herrera M, Kerick M, et al. GWAS for systemic sclerosis identifies multiple risk loci and highlights fibrotic and vasculopathy pathways. Nat Commun. 2019;10(1):4955.
Acknowledgments: NIL.
Disclosure of Interests: Carlos Rangel-Peláez: None declared, Carlos Rosa-Baez: None declared, Inmaculada Rodriguez-Martin: None declared, Martin Kerick: None declared, Alfredo Guillen-Del-Castillo: None declared, Carmen P. Simeón-Aznar: None declared, José Luis Callejas: None declared, Alexandre Voskuyl: None declared, Alexander Kreuter: None declared, Oliver Distler: None declared, International SSc Group: None declared, Susanna M. Proudman: None declared, Mandana Nikpour: None declared, Australian Scleroderma Interest Group (ASIG): None declared, Nicolas Hunzelmann: None declared, Gianluca Moroncini: None declared, Armando Gabrielli: None declared, Jörg Distler: None declared, Jeska K. de Vries-Bouwstra Speaker fees from Janssen-Cilag, Boehringer-Ingelheim, Pfizer, Astra-Zeneca, BMS, UCB, Novartis, Abbvie, Lilly, alfsigma; all payments are made to her institution, Consultancy fees from Janssen-Cilag, Boehringer-Ingelheim, Abbvie; all payments are made to her institution, Research grants from Galapagos, Vifor, Janssen-Cilag, ReumaNederland, NVLE; all payments are made to her institution, Ariane L. Herrick: None declared, Yannick Allanore: None declared, Lorenzo Beretta: None declared, Brian Skaug: None declared, Shervin Assassi Speaking fees from Boehringer Ingelheim., Consultancy fees from Abbvie, aTyr, AstraZeneca, Boehringer Ingelheim, Bymmunity, Candid, CSL Behring, Merck, Mitsubishi Tanabe, Takeda and UCB, Research grants from Abbvie, aTyr, Boehringer Ingelheim and Janssen, Christopher P. Denton: None declared, Javier Martin: None declared, Lourdes Ortiz-Fernández: None declared, Marialbert Acosta-Herrera: None declared.