fetching data ... 
Background: Gout is a chronic inflammatory disease caused by deposition of monosodium urate crystals. Recurrent acute flares represent a major challenge in gout management and lead to significant clinical and economic burden. Despite the potential of urate-lowering therapy to “cure” gout, poor adherence and unpredictable flare patterns hinder effective long-term management.
Objectives: This study aimed to develop and validate a multimodal artificial intelligence model that integrates structured laboratory data with unstructured clinical text from electronic health records (EHRs) to predict the risk of acute gout flares.
Methods: We conducted a retrospective cohort study using EHRs from Daping Hospital of Army Medical University (Third Military Medical University) in Chongqing, China. Following the application of inclusion and exclusion criteria, a final cohort of 8983 patients with gout was established. From this cohort, both structured data (e.g., laboratory results) and unstructured clinical notes were subsequently extracted. The textual data were processed using the MedBERT model to generate semantic embeddings, which were subsequently reduced in dimensionality via singular value decomposition (SVD). For prediction, a multimodal architecture was designed: a Transformer-based network handled the text data, while tree-based algorithms (XGBoost, LightGBM, CatBoost) analyzed the structured data. Predictions from these individual models were then fused using a Stacking-integrated Meta model. The entire framework was trained and evaluated using stratified 5-fold cross-validation, with performance assessed by standard metrics including AUC, accuracy, precision, recall, and F1-score.
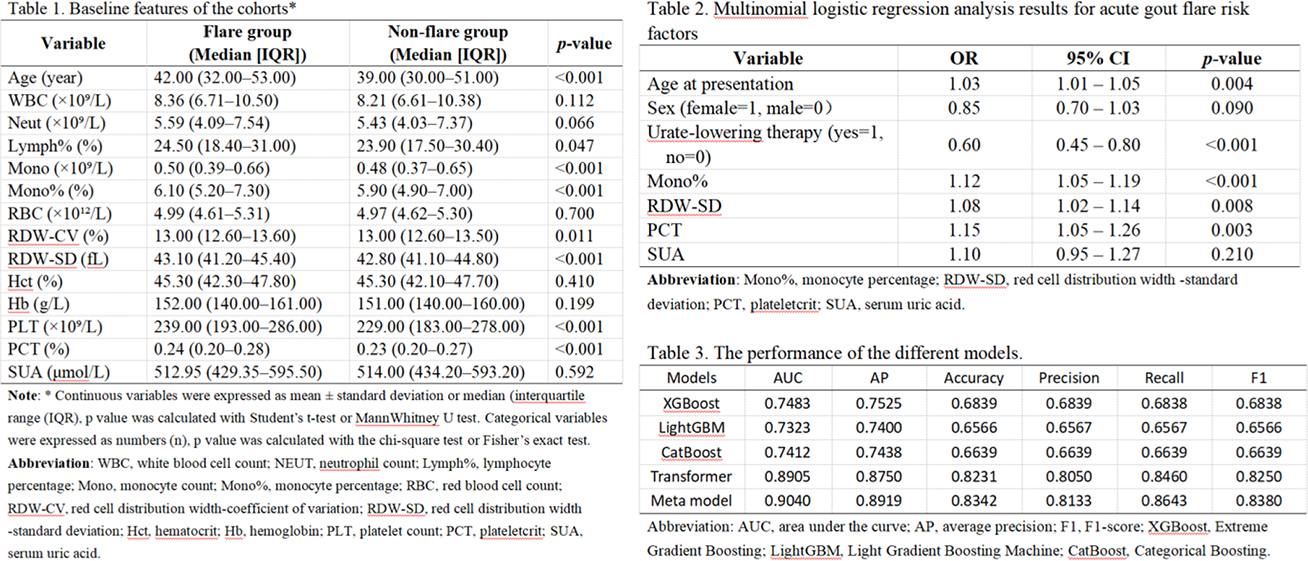
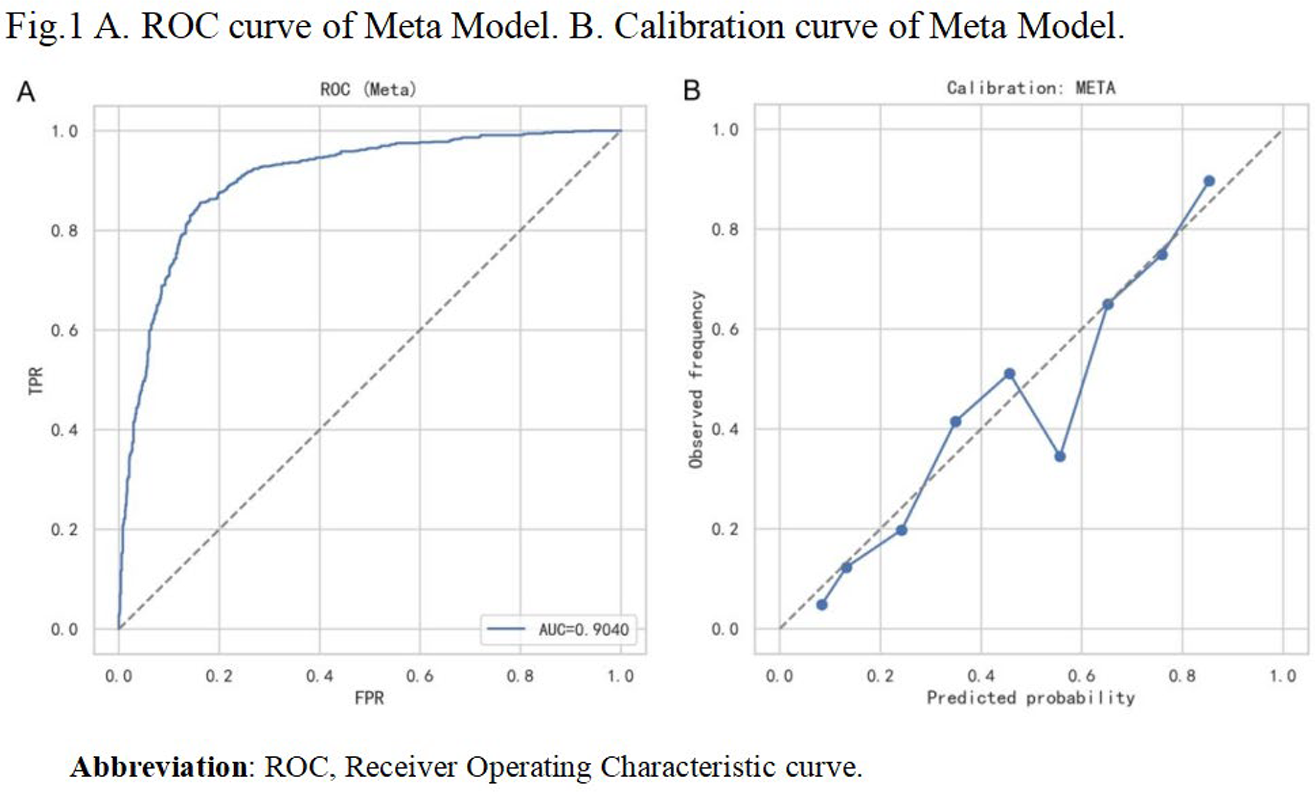
Results: Significant differences were observed in age (median age 42.0 vs. 39.0 years, p<0.001), monocyte counts and percentages, red cell distribution width - standard deviation (SD), platelet counts, and plateletcrit between flare and non-flare groups (p<0.001, Table 1). However, serum uric acid levels showed no significant difference between groups (p=0.592, Table 1). Multivariate analysis confirmed these variables as independent predictors (Table 2): age (OR=1.03, 95% CI 1.01-1.05), monocyte percentage (OR=1.12, 95% CI 1.05-1.19), red cell distribution width-SD (OR=1.08, 95% CI 1.02-1.14), and plateletcrit (OR=1.15, 95% CI 1.05-1.26). Whereas long-term regular urate-lowering therapy was protective (OR=0.60, 95% CI 0.45-0.80). When modeling these features, the Transformer-based text model significantly outperformed those using only structured data, achieving an AUC of 0.8905 compared to 0.7483 for XGBoost (Table 3). Furthermore, the multimodal Meta model surpassed all single-modality approaches, achieving a test AUC of 0.9040, with an average precision of 0.8919, an accuracy of 0.8342, and a recall of 0.8643 (Table 3, Figure 1A). This model demonstrated robust calibration, indicating high agreement between predicted probabilities and observed outcomes (Figure 1B).
Conclusions: Our multimodal prediction model, by synthesizing structured and unstructured EHR data, provides a robust tool (AUC > 0.90) for predicting acute gout flares, outperforming models based on single data modalities. This strategy shows promise for enabling proactive flare management, though further validation is needed to assess clinical implementation potential.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.