fetching data ... 
Background: Systemic sclerosis-associated pulmonary arterial hypertension (SSc-PAH) is a heterogeneous disease with an unpredictable clinical course. Current follow-up relies on comprehensive hospital-based assessments, in which World Health Organization functional class (WHO-FC), 6-minute walk distance (6MWD), and NT-proBNP are key parameters used to evaluate disease status and prognosis. Fixed-interval hospital follow-up may be insufficient to capture early and clinically relevant changes, and digital home monitoring offers the opportunity for more frequent assessment. However, data on the feasibility and validity of home-based assessments in SSc-PAH remain limited.
Objectives: The primary objective was to evaluate the feasibility of implementing a digital home-monitoring programme in patients with SSc-PAH. Specific aims were to assess selected home-based measures by comparison with standard hospital-based assessments, as well as patient adherence, satisfaction, and usability.
Methods: This prospective open-label clinical pilot trial (ClinicalTrials.gov identifier: NCT06865118) enrolled patients with SSc-PAH, defined according to the 2022 ESC/ERS haemodynamic criteria. The study was approved by the relevant ethics committee, and all participants provided written informed consent. Patients participated in a 12-week digital home-monitoring programme conducted between March and June 2025. Home monitoring was conducted via a secure digital platform (Zeen Health) specifically developed for SSc-PAH and included biweekly patient-reported symptom assessments using the modified Medical Research Council (mMRC) dyspnoea scale and visual analogue scales (VAS) covering cardiopulmonary symptom burden. Functional assessment was performed using a one-minute sit-to-stand test (1MSTS) with continuous pulse oximetry, and exertional dyspnoea was assessed using the Borg scale. A set of validated patient-reported outcome measures was completed at baseline and study completion: EmPHasis-10, EQ-5D-5L, ScleroID, Hospital Anxiety and Depression Scale (HADS), and Health Assessment Questionnaire (HAQ). Patient satisfaction and usability were assessed at the end of the study using the Client Satisfaction Questionnaire (CSQ-8) and a study-specific questionnaire, with responses summarised descriptively for visualisation. Hospital-based assessments were performed at baseline and week 12 and included clinical evaluation, pulmonary function testing, ECG, laboratory testing (including venous and capillary NT-proBNP), and functional assessment with 6MWD and 1MSTS. Echocardiography was performed at baseline. To evaluate selected home-based measures, associations with corresponding hospital-based assessments were analysed using Spearman’s rank correlation, and agreement between home- and hospital-based 1MSTS was assessed using Bland-Altman analysis. Adherence was defined as the proportion of completed home-monitoring assessments relative to those scheduled.
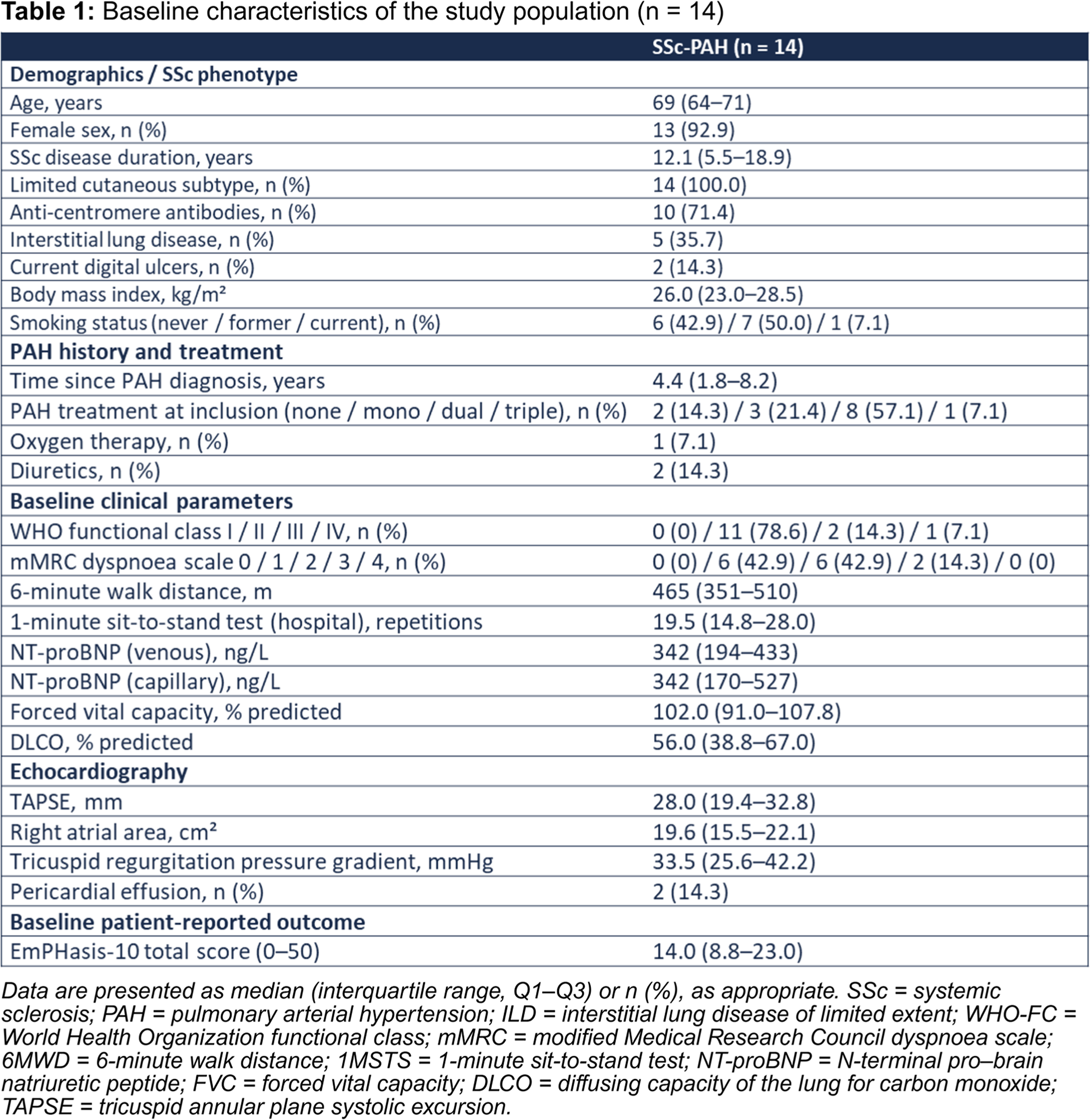
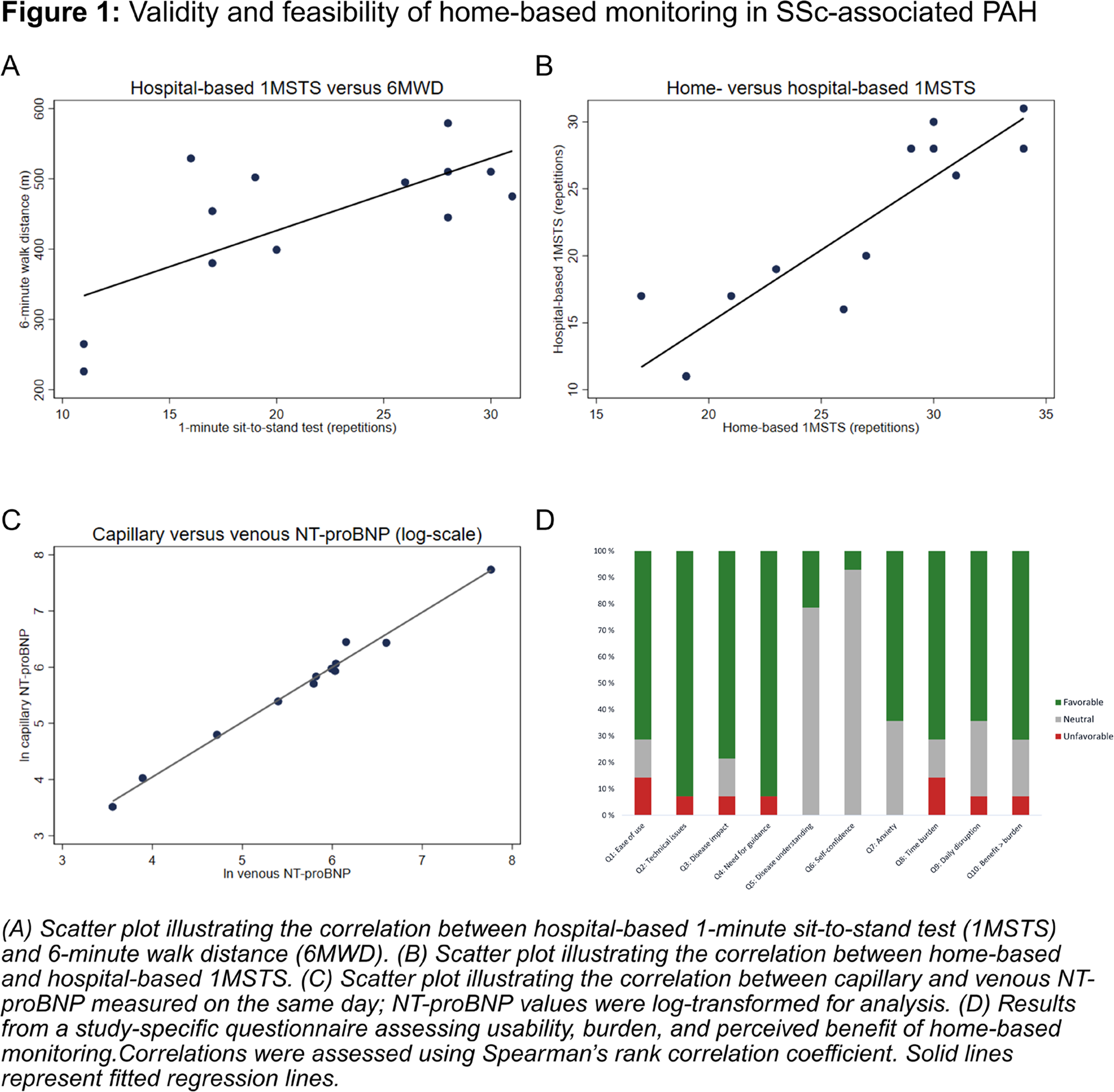
Results: Fourteen patients with SSc-PAH were included (median age 69 years; 93% female); all had limited cutaneous SSc, and the median time since PAH diagnosis was 4.4 years. Most patients were in WHO-FC II (78.6%), with fewer in class III (14.3%) and IV (7.1%). Median 6MWD was 465 m, and median venous NT-proBNP was 342 ng/L (Table 1). When comparing home-based measures with corresponding hospital-based assessments, hospital-based 1MSTS repetitions were moderately correlated with 6-minute walk distance (Spearman’s ρ = 0.61, p = 0.023; Figure 1A), supporting the validity of 1MSTS as a measure of functional capacity. Home- and hospital-based 1MSTS were strongly correlated (Spearman’s ρ = 0.86, p = 0.0005; Figure 1B). Bland–Altman analysis demonstrated a systematic difference, with home-based testing yielding on average 4.5 higher repetitions, but no evidence of proportional bias. Patient-reported dyspnoea using the mMRC scale showed a moderate, non-significant correlation with physician-assessed WHO-FC (Spearman’s ρ = 0.49, p = 0.08). Capillary NT-proBNP levels strongly correlated with venous NT-proBNP measured on the same day (Spearman’s ρ = 0.99, p < 0.001; Figure 1C). To assess patient adherence, satisfaction and usability, a total of 98 home-monitoring assessments were scheduled, of which 94 were completed, corresponding to an overall adherence of 96%. Thirteen patients completed all scheduled assessments, while one patient completed three of seven. During follow-up, 39 patient-study team contacts were recorded, including 17 patient-initiated contacts. Of these, seven concerned technical issues, mainly related to login or connectivity, wearable device handling, or data registration, and were resolved with guidance from the study team. Study-initiated contacts primarily concerned reminders related to missing entries and logistical or procedural clarifications. The median CSQ-8 total score was 26.5 out of a maximum of 32 (IQR 24.0–30.0), indicating high satisfaction. In a complementary study-specific questionnaire addressing usability, burden, and perceived benefit of home monitoring, most participants reported easy use, infrequent technical issues, low burden, and limited anxiety related to monitoring, and agreed that the perceived benefits outweighed potential disadvantages (Figure 1D).
Conclusions: In this pilot study, a digital home-monitoring programme in patients with SSc-PAH was feasible and well accepted by patients, with high adherence and patient satisfaction. Measures reflecting functional capacity, symptom burden, and biomarkers showed overall associations with corresponding established clinical assessments, supporting the potential of digital home monitoring to complement standard hospital-based follow-up. These findings suggest that selected home-based measures may enable more frequent assessment of disease status outside the hospital setting.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Hilde Jenssen Bjørkekjær Janssen, Maylen N Carstens: None declared, Peter Andel SOBI, Novartis og BMS, Håvard Fretheim: None declared, Kastriot Kastrati Boehringer Ingelheim, Novartis, UCB Pharma, Sandos, Eli Lilly and AbbVie, Emily Langballe: None declared, Phuong Phuong Diep Boehringer-Ingelheim, Boehringer-Ingelheim and NordicInfu Care AB, Boehringer-Ingelheim (institutional research grant), Marthe Mæhlen: None declared, Torhild Garen: None declared, Cathrine Brunborg: None declared, Mona Lovise Talaro Ramsli: None declared, Helle Bitter: None declared, Sverre Høie: None declared, Arne Andreassen: None declared, Kaspar Broch Amgen, Astra, Bayer, Boehringer, Novartis, Novo Nordisk, Pharmacosmos, and Pfizer, Øyvind Molberg: None declared, Anna-Maria Hoffmann-Vold Boehringer Ingelheim, Janssen, Medscape, Merck Sharp & Dohme, Novartis, Roche, AbbVie, Avalyn, Astra Zeneca, Boehringer Ingelheim, Bristol Myers Squibb, Calluna Pharma, Genentech, Janssen, Medscape, Merck Sharp & Dohme, Pliant, Roche, Werfen, Astra Zeneca, Boehringer Ingelheim, Janssen.