fetching data ... 
Background: Interstitial lung disease (ILD) is a major cause of morbidity and mortality in systemic sclerosis (SSc). High-resolution CT (HRCT) is central to ILD assessment, yet qualitative interpretation is limited by interobserver variability and low sensitivity to subtle changes. Artificial intelligence (AI)–based quantitative HRCT tools may improve reproducibility and prognostic accuracy. Contextflow ADVANCE Chest CT provides automated quantification of radiologic abnormalities, but its clinical utility in SSc-ILD has not been fully evaluated.
Objectives: To assess the prognostic value of an AI-derived HRCT abnormality score in SSc-ILD, including its association with pulmonary function decline, radiologic progression, and 5-year mortality, and to evaluate whether immunomodulatory treatments influence radiologic outcomes.
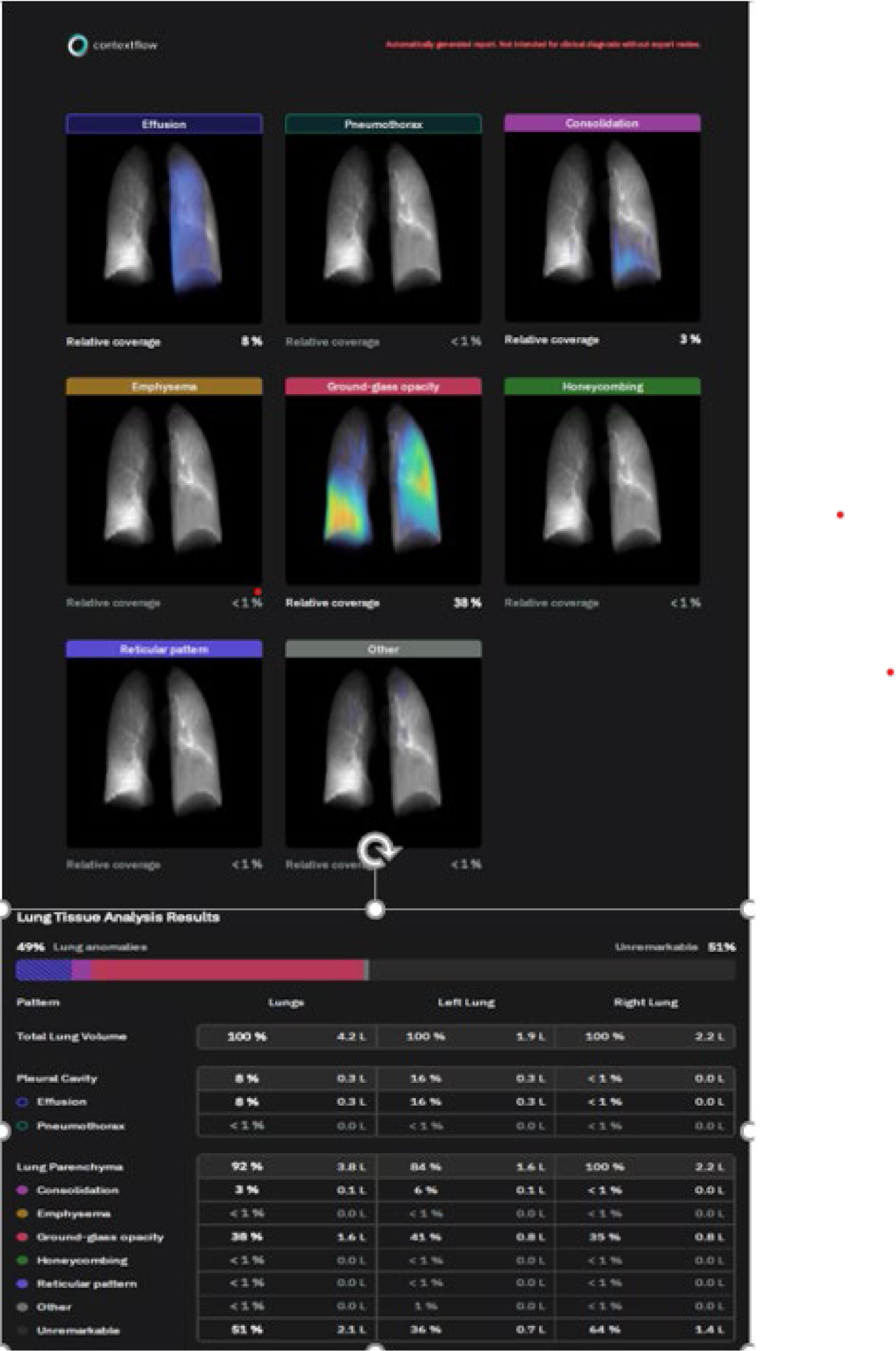
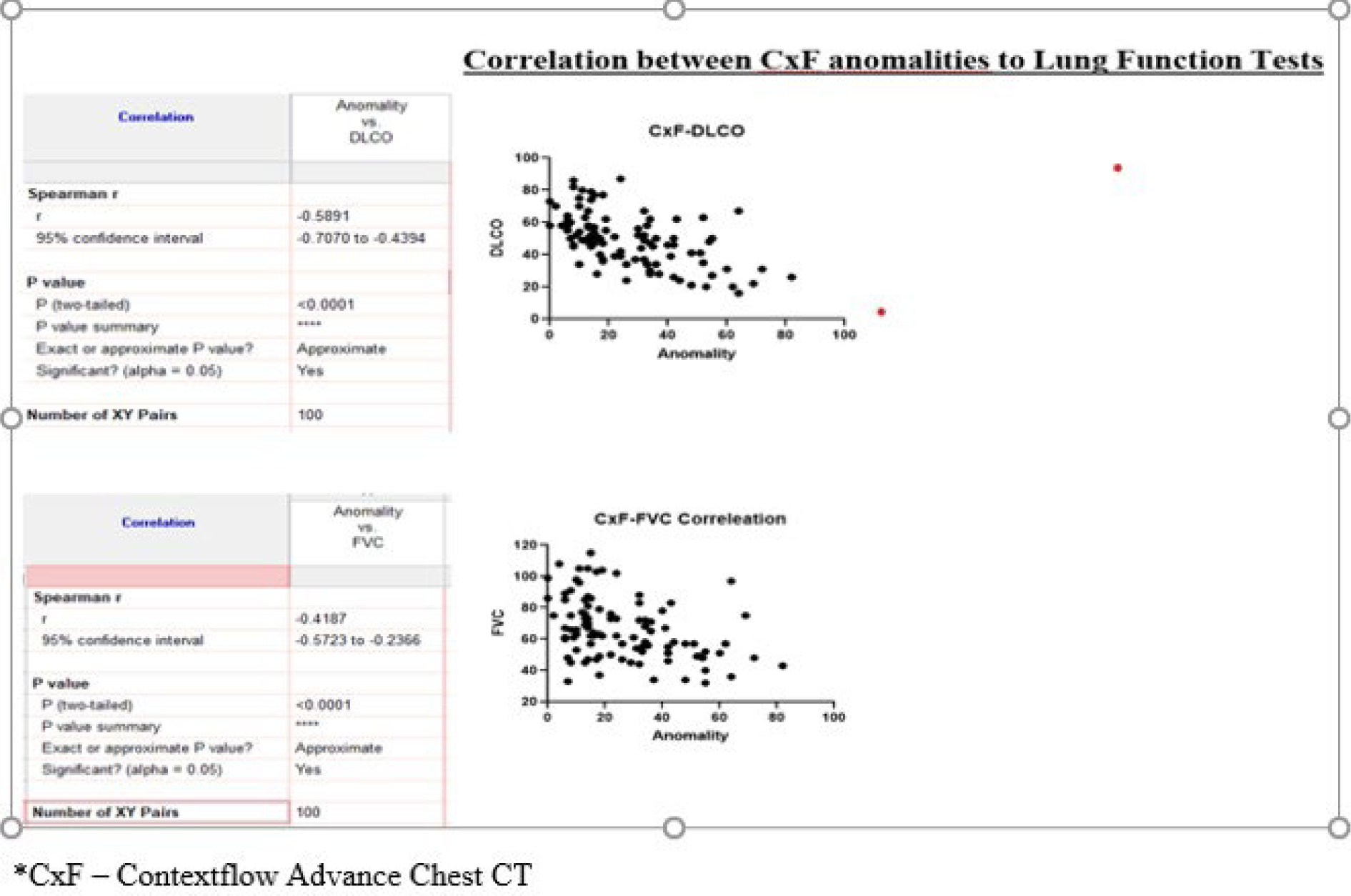
Methods: A retrospective cohort study was conducted using a prospectively maintained database of SSc patients followed at a tertiary center between 2006 and 2024. Patients were included if they had ≥2 HRCT scans, serial pulmonary function tests (PFTs), and ≥3 years of follow-up. HRCT scans were analyzed using Contextflow ADVANCE Chest CT to generate a weighted lung abnormality score (QILD) (image 1). Correlations between baseline QILD and subsequent PFTs were assessed using Spearman’s coefficients. Associations with 5-year mortality were evaluated using Fisher’s exact test. Radiologic progression was compared across treatment groups (mycophenolate mofetil, cyclophosphamide, rituximab) using Mann-Whitney tests.
Results: Of 450 SSc patients, 67 met inclusion criteria. Mean age at diagnosis was 44.7 years; 83.6% were female and 73.1% had diffuse cutaneous SSc. Anti-Scl70 antibodies were present in 67.2%. Baseline mean FVC was 69% predicted and DLCO 54% predicted. The mean QILD score was 25.5, with ground-glass opacities as the predominant abnormality. During a mean follow-up of 11.1 years, 39% of patients showed radiologic progression, 33% showed improvement, and 39% died. Baseline QILD correlated significantly with PFTs obtained ≥3 years later (FVC: p=0.029; DLCO: p=0.029). No significant association was observed between specific immunomodulatory treatments and short-term radiologic change. A baseline QILD score >20 was associated with significantly higher 5-year mortality (19.5% vs. 4.8%; p=0.048), corresponding to a four-fold increased risk.
Conclusions: An AI-derived HRCT abnormality score provides meaningful prognostic information in SSc-ILD. Higher baseline QILD scores predict long-term pulmonary function decline and increased 5-year mortality. Although radiologic response did not differ across treatment groups, the findings support integrating quantitative AI-based HRCT analysis into routine assessment and risk stratification of SSc-ILD. Prospective studies are needed to refine its role in guiding therapeutic decisions
Example of an output report generated by Contextflow ADVANCE Chest CT analysis.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: None declared.