fetching data ... 
Background: Giant cell arteritis (GCA) is the most frequent vasculitis after 50 years old. Induction treatment is based on steroids. Relapses are frequent, occurring in half of the patients, resulting in prolonged steroids use. GCA patients are exposed to long term steroids side effects. To limit those adverse events, several Disease Modifying Anti-Rheumatic Drugs (DMARDS) have been studied for their steroid-sparing effect. There is still an unmet need to identify patients at risk for relapse in GCA [1,2]. Patients at higher risk could be eligible to early immunosuppressive treatment. Clonal hemopoiesis of indeterminate prognosis (CHIP) is defined as detection of somatic mutation in bone marrow or peripheral blood, without criteria for myelodysplastic syndrome or myeloproliferative neoplasms [3]. CHIP prevalence is increasing with age with 20% at 80 years-old. Population-based studies reported association between CHIP and cancer, cardio-vascular diseases, and some inflammatory process [3,4]. Some studies reported a higher CHIP prevalence in patients with GCA [5].
Objectives: Our objective was to assess CHIP association with GCA relapse. Secondary objective was to study if CHIP was associated with specific GCA presentation at diagnosis.
Methods: We prospectively analyzed CHIP in a monocentric cohort of recent diagnosed GCA patients. CHIP was defined as a variant allelic frequency > 2% detected in peripheral blood mononuclear cells by next-generation sequencing. Relapses were defined as GCA related symptoms or inflammatory syndrome after remission induction. Primary outcome was relapse occurring within 12 months of GCA induction treatment.
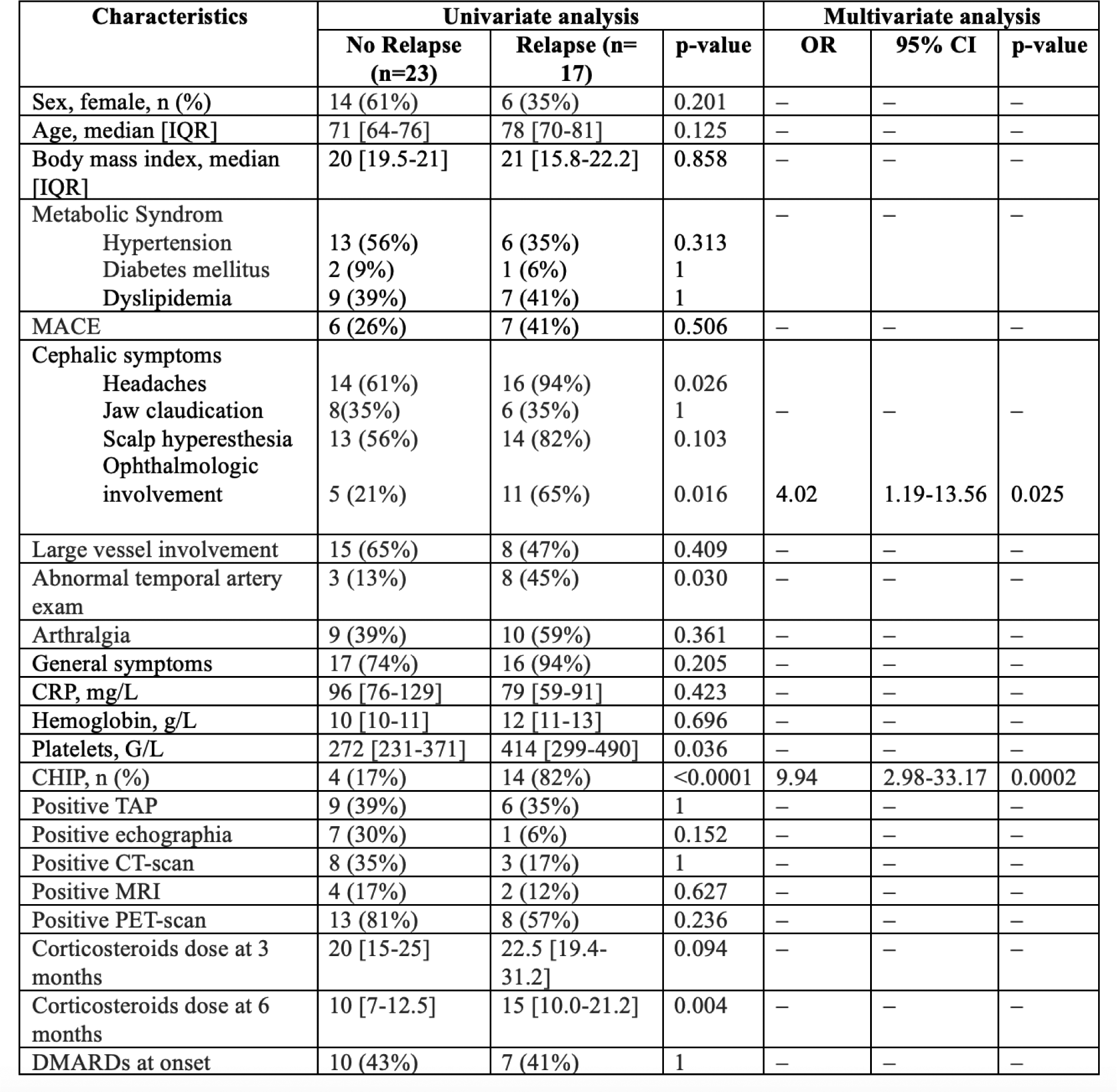
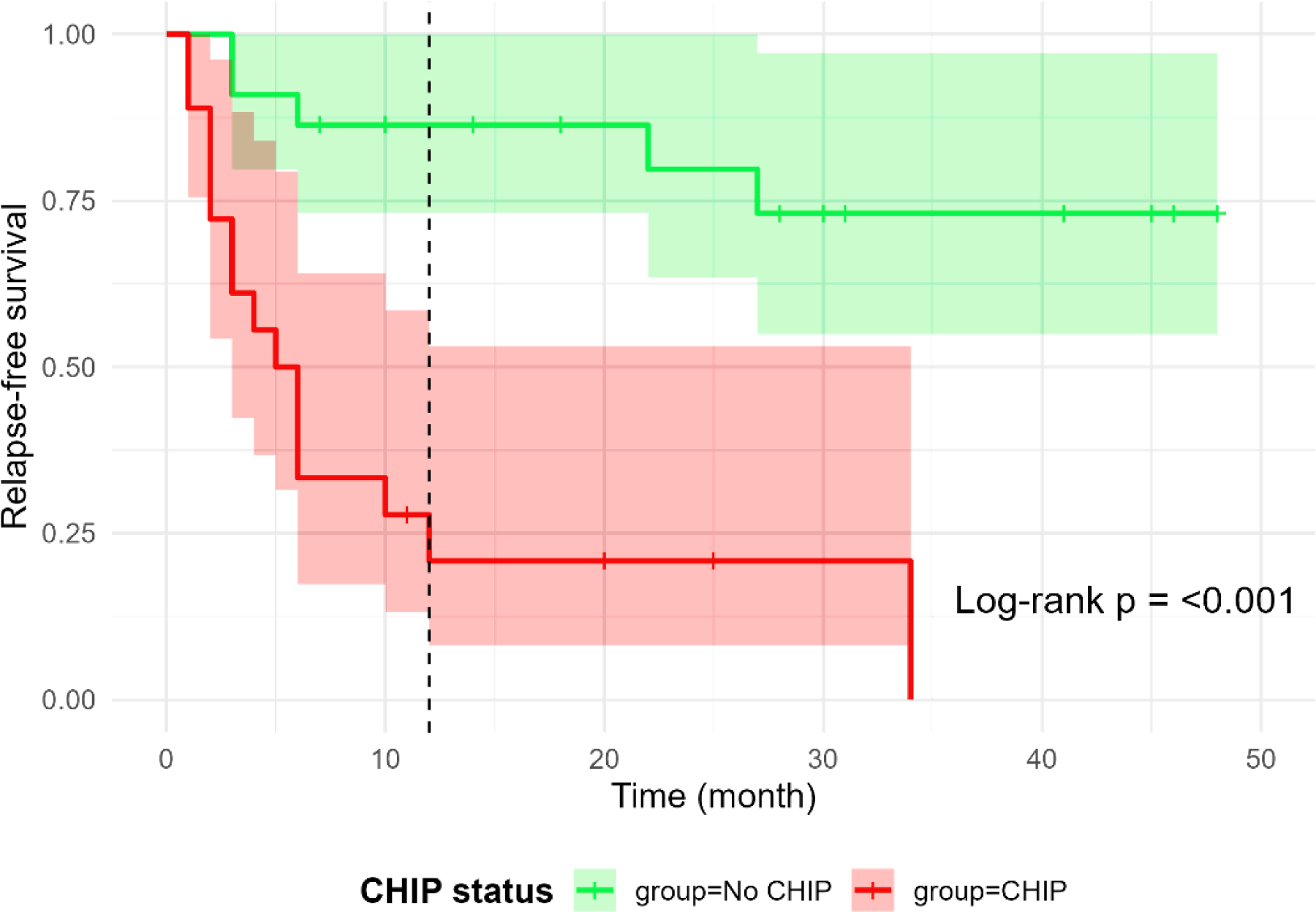
Results: During the study period, we included 40 patients, median age 73 [67-80] years-old, including 20 (50%) women. At diagnosis, 34 (85%) patients had cephalic phenotype with headaches in 30 (75%) patients, 16 (40%) patients had ophthalmic involvement, and 23 (57%) patients had large vessel involvement. Temporal artery biopsy was performed in 31 (77%) patients, positive in 15 (48%). All patients received steroids at diagnosis, and 17 (43%) patients received steroids-sparing strategies, 7 (17%) with anti-IL6 therapy and 6 (15%) with methotrexate et 4 (10%) patients with anti-IL17. CHIP was detected in 18 (45%) patients, including 11 patients with one mutated clone, 7 with two mutated clones, and 3 with three mutated clones. Median VAF was 4% [2-11] and most prevalent mutated clones were TET2 in 6 patients and DNMT3A in 5 patients. In univariate analysis, major adverse cardiac events (MACE) [4 (18%) in no CHIP patients vs. 9 (50%) in CHIP patients, p=0.05] were associated with CHIP. No GCA features at diagnosis were different between no CHIP and CHIP patients. During a median follow-up of 26 months [14-45], 20 (50%) patients relapsed, including 17 (42%) relapses during the first year after diagnosis. GCA manifestations at relapse were similar to those at disease onset in 13 (72%) patients. All relapses were treated by steroids increase. Anti-IL6 treatment was initiated after relapse in 15 patients (37%) and methotrexate in 1 case (2%). In univariate analysis, patients with relapse at M12 presented headaches at diagnosis [14 (61%) patients in no relapse group vs. 16 (94%) in relapse group, p=0.03], had more frequently ophthalmologic involvement at diagnosis (5 (22%) patients in no relapse group vs. 11 (65%) patients in relapse group, p=0.02), higher neutrophil and platelets count at diagnosis (respectively 4.9 [3.8-6.3]G/L vs. 8.3 [6.2-9.8] G/L, p=0.02 and 272 [231-371]G/L vs. 414 [299-490] G/L, p=0.04 for neutrophils and platelet in no relapse group and relapse group, respectively), and were more frequently CHIP positive (4 (17%) vs. 14 (82%), p=< 0.0001). In multivariate analysis, factors independently associated with relapse were ophthalmologic involvement (OR 4.02, CI95% [1.19-13.56], p <0.025) and CHIP (OR 9.94, CI95% [2.98-33.17], p=0.0002). Patients with CHIP had more frequent and earlier relapses (p=0.0001). Adverse events were reported in 24 (67%) patients, infectious disease were predominant with 16 (41%) patients, followed by rheumatologic adverse event in 11 (28%). Three severe adverse events (8%) were reported (1 urinary tract infection with septic shock, 1 chorioretinitis with ophthalmologic sequela and 1 pulmonary embolism). Vascular adverse events occurred in 11 (61%) patients, including 3 strokes (8%), 10 cases of stenosis/sub occlusion (28%), 4 aneurysms (11%) and 1 vascular dissection (3%). No death was observed during the timeline of the study.
Conclusions: In conclusion, this study identifies CHIP as an independent predictor of relapse in GCA. Screening for CHIP at diagnosis could improve risk stratification and inform individualized therapeutic strategies.
Table 1. Characteristics of relapse in univariate and multivariate analysis.
Relapse Free Survival in giant cell arteritis patients according to CHIP status
REFERENCES: [1] C D, et al. Giant cell arteritis and polymyalgia rheumatica: current challenges and opportunities. Nature reviews Rheumatology [Internet]. 2017 Oct [cited 2025 Jul 26];13(10). Available from:
[2] D P, et al. Large-vessel vasculitis. Nature reviews Disease primers [Internet]. 2022 Jun 1 [cited 2025 Jul 26];7(1). Available from:
[3] J S, et al. Clonal hematopoiesis of indeterminate potential as a prognostic factor: a systematic review and meta-analysis. Blood advances [Internet]. 2024 Jul 23 [cited 2025 Jul 27];8(14). Available from:
[4] Köhnke T, et al. Clonal hematopoiesis: from mechanisms to clinical intervention. Cancer Discov. 2021 Dec 1;11(12):2987–97.
[5] F GR, et al. Clonal haematopoiesis across the age spectrum of vasculitis patients with Takayasu’s arteritis, ANCA-associated vasculitis and giant cell arteritis. Annals of the rheumatic diseases [Internet]. 2024 Dec 3 [cited 2025 Jul 27];83(4). Available from:
Acknowledgments: NIL.
Disclosure of Interests: None declared.