fetching data ... 
Background: In polymyalgia rheumatica (PMR), frailty may develop through the interplay of systemic inflammation, functional impairment, age-related vulnerability, and glucocorticoid exposure. Despite growing interest in frailty across inflammatory rheumatic diseases, its longitudinal trajectory, determinants, and clinical relevance in PMR remain poorly characterised.
Objectives: To characterise changes in frailty status over 12 months in patients with PMR, identify predictors of frailty progression, and examine associations between frailty status, disease outcomes, and patient-reported outcomes (PROs).
Methods: This multicentre, longitudinal cohort study included participants with newly diagnosed isolated PMR, recruited through a fast track PMR clinic. Frailty was assessed at baseline and 12 months using the Fried frailty phenotype. Baseline demographic and clinical data were collected at baseline, with longitudinal follow-up at 12 months for frailty outcomes and at 18 months for relapse outcomes. Paired changes in frailty components were assessed using exact McNemar’s, Wilcoxon signed-rank, or paired t-tests as appropriate. Logistic regression models were used to identify predictors of frailty at 12 months, and relapse at 18 months. Non-parametric tests compared PROs across frailty categories, with all statistical analysis performed in R version 4.3.3 (R Core Team, 2024).
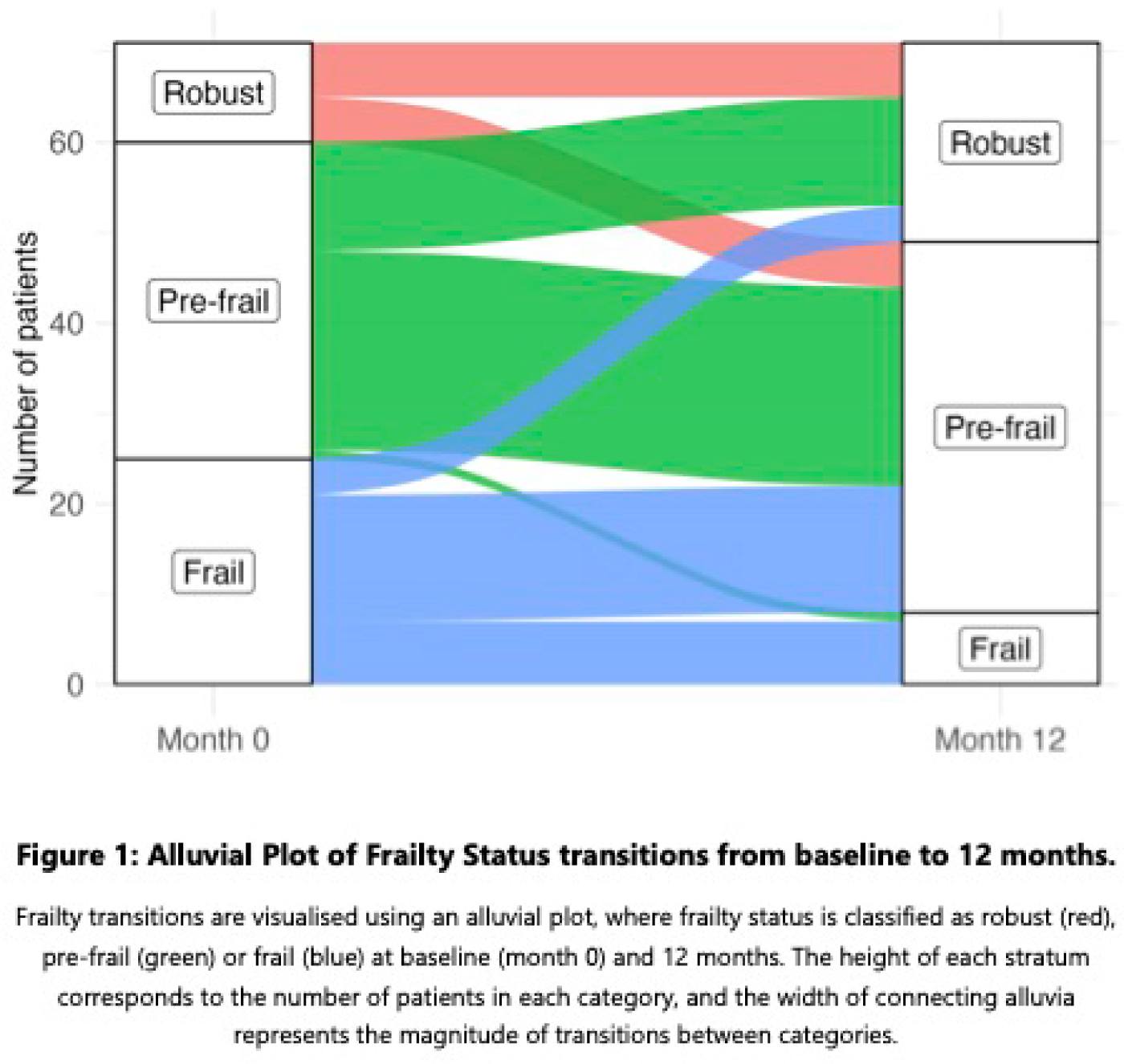
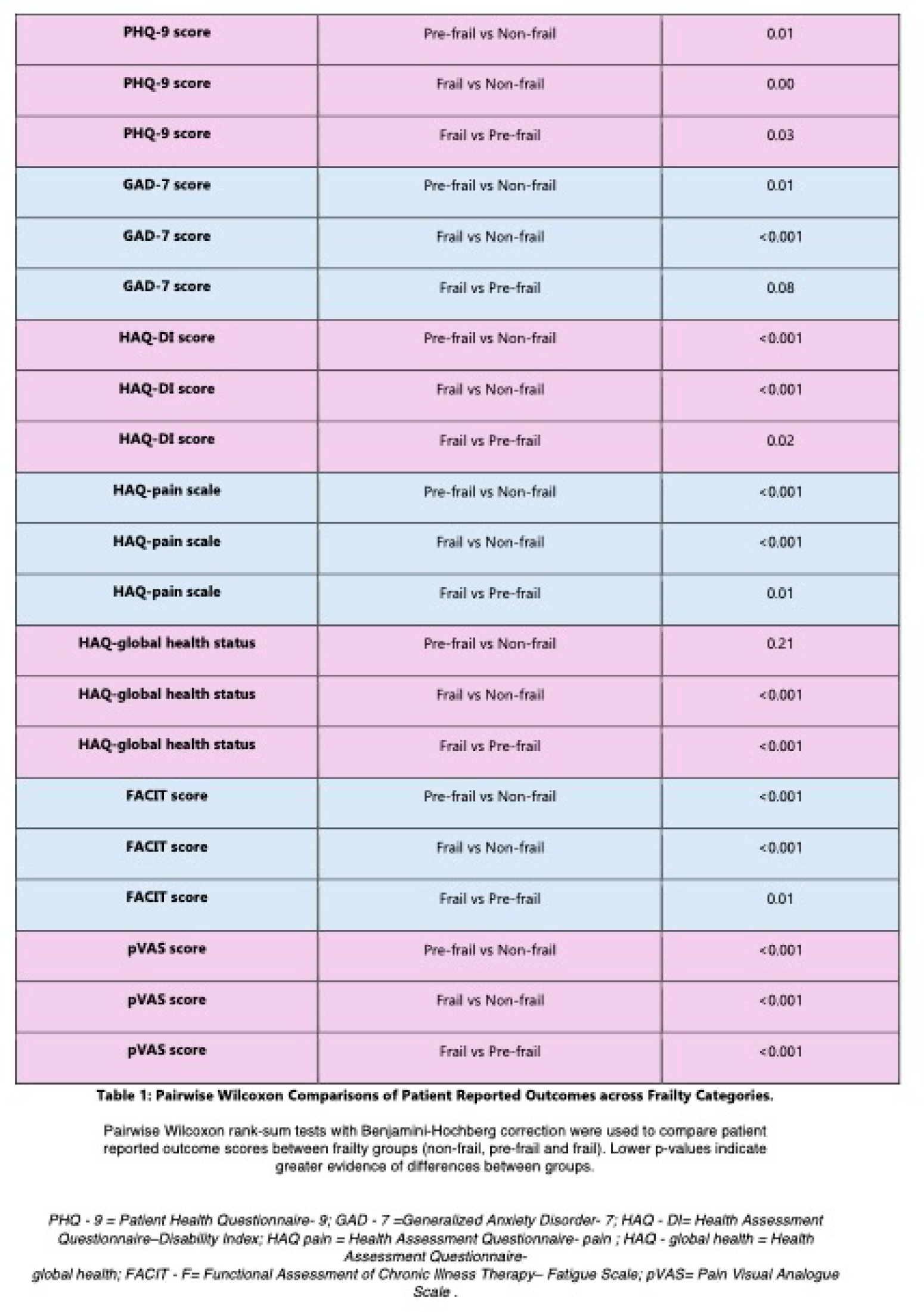
Results: 71 participants, 47.9% (n=34) females, with a mean age of 71.0 years (SD 7.62) were included. At baseline, 15.5% (n=11) were robust, 49.3% (n=35) were pre-frail, and 35.2% (n=25) were frail. Over 12 months, 49.3% maintained their baseline frailty state, 42.3% improved, and 8.5% worsened. At 12 months, 31% (n=22) were robust, 57.7% (n=41) were pre-frail and 11.3% (n=8) were frail. Marked improvements were observed in several frailty components, including the prevalence of weight loss, which declined from 23.9% to 1.4% (p<0.001), slowness from 33.8% to 12.7% (p<0.001) and exhaustion from 62.0% to 22.5% (p<0.001). Low physical activity showed a non-significant trend toward improvement 33.6% to 22.5%; p=0.064. In contrast, the prevalence of reduced hand grip strength increased from 49.3% (n=35) to 63.4% (n=45) (p=0.076), with the mean handgrip (kg) decreasing from 26.3 (SD 11.4) to 23.4 (SD 9.7); p=0.04. In univariable analysis, higher baseline BMI (OR 1.11 per unit BMI, 95% CI 1.01-1.22, p=0.037), higher PMR activity score (PMR-AS) at 12 months (OR 1.11 per point increase, 95% CI 1.03-1.20, p=0.0045) and higher cumulative steroid exposure at 12 months (OR 1.00, 95% CI 1.0-1.0, p<0.01) were associated with increased frailty status at 12 months. Female sex and higher comorbidity burden showed non-significant trends towards increased frailty, whilst age was not associated. In multivariable models, BMI (OR 1.13, 95% CI 1.06-1.21; p<0.001) and PMR-AS (OR 1.13; 95% CI 1.05-1.22; 0=0.002) remained significant whilst cumulative steroid exposure lost significance (p=0.26). Baseline frailty status predicted relapse at 18 months. Pre-frail participants had significantly higher odds of relapse compared with robust individuals (OR=5.11, 95% CI 1.23-26.79; p=0.03), while frail participants also demonstrated increased odds, although this did not reach statistical significance (OR=3.39, 95% CI 0.78-18.43; p=0.12). Frailty was strongly associated with worse PROs, including pain (pVAS), fatigue (FACIT-F), mood (PHQ-9), anxiety (GAD-7) and health related quality of life (HAQ-DI), in a dose dependent manner. Frail patients consistently reported the poorest scores, pre-frail participants intermediate scores, and non-frail participants the most favourable scores (Table 1), with two exceptions for GAD-7, frail and pre-frail patients did not differ significantly (p=0.08), and for HAQ-Global health, non-significant difference was found between pre-frail and non-frail patients (p=0.21).
Conclusions: In PMR, increased frailty is highly prevalent and clinically meaningful. Although frailty status improved in many patients over 12 months, driven largely by improvements in symptom related components, a substantial proportion remained pre-frail or frail, and muscle strength showed a tendency to worsen. Frailty was independently associated with ongoing disease activity, higher BMI and markedly worse PROs including pain, fatigue, depression, anxiety and overall health related quality of life. Moreover, pre-frailty was identified as a significant predictor of relapse risk up to 18 months. Our findings underscore the importance of frailty monitoring across all patients with PMR, in order to modify frailty trajectories, reduce adverse outcomes and improve quality of life in those with PMR.
REFERENCES: NIL.
Acknowledgments: NIL.
Disclosure of Interests: Patricia Harkins Johnson and Johnson, Novartis, Sharon Cowley Novartis, Danielle Molloy: None declared, David Kane: None declared, Richard Conway: None declared.