fetching data ... 
Background: Takayasu arteritis is a systemic, autoimmune vasculitis of the large vessels, primarily affecting the aorta and its major branches. A subset of Takayasu arteritis begins in the child age group, yet the differences in clinical manifestations and long-term prognosis between juvenile-onset and adult-onset remain unclear. Although specific Human Leukocyte Antigens (HLA), such as HLA-B52, are known to be associated with susceptibility to Takayasu arteritis, the precise HLA characteristics of juvenile-onset Takayasu arteritis remain unknown. Furthermore, juvenile-onset Takayasu arteritis patients face a high risk of organ damage due to prolonged glucocorticoid (GC) use over a long disease duration, making the achievement of GC-free remission an ideal therapeutic goal.
Objectives: Therefore, this study aimed to investigate the differences in clinical manifestations, including HLA-B profiles, between juvenile- and adult-onset Takayasu arteritis and to clarify the long-term prognosis, specifically the rate of GC-free remission.
Methods: Patients with Takayasu arteritis attending Kyoto University Hospital between 2018 and 2024 were enrolled in this study. Inclusion criteria were: disease onset before 60 years of age, a minimum disease duration of three years, and a history of GC treatment. All patients fulfilled the 2010 European Alliance of Associations for Rheumatology (EULAR)/Paediatric Rheumatology International Trials Organization (PRINTO)/Paediatric Rheumatology European Society (PRES) classification criteria [1]. Patients were stratified into two groups: juvenile-onset (≤18 years) and adult-onset (>18 years). First, differences in clinical characteristics and HLA-B profiles between the juvenile- and adult-onset groups were assessed using the Mann-Whitney U test for continuous variables and Fisher’s exact test for categorical variables. The associations between juvenile-onset and characteristics/HLA were further analyzed using logistic regression. Second, the 30-year cumulative GC-free remission rates were analyzed by comparing the juvenile- and adult-onset groups. Prognosis was assessed using Kaplan-Meier survival curves and log-rank tests. Cox proportional hazard analyses for the continuous use of GC, adjusted for observation periods, were performed to determine the factors contributing to GC-free status.
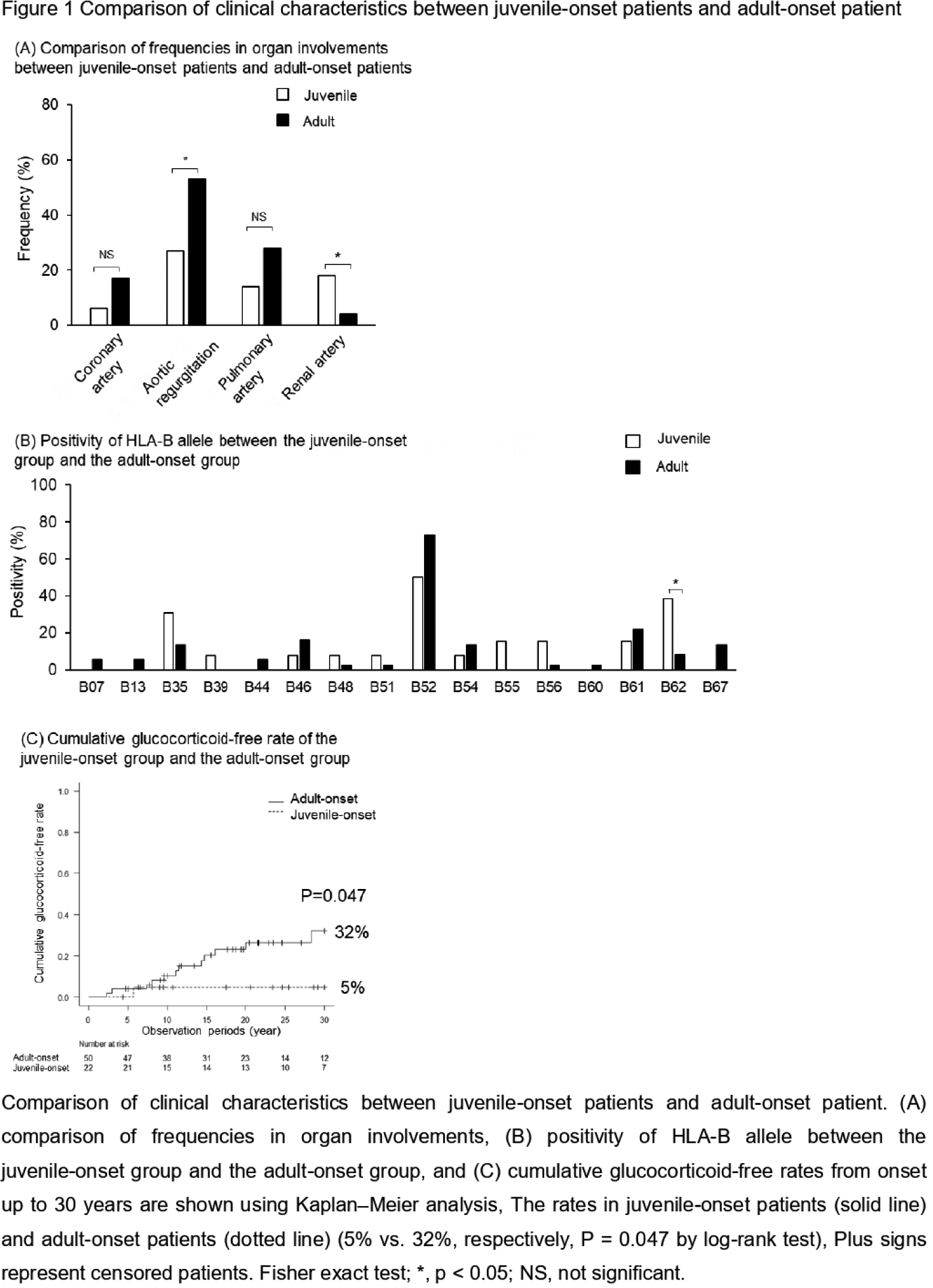
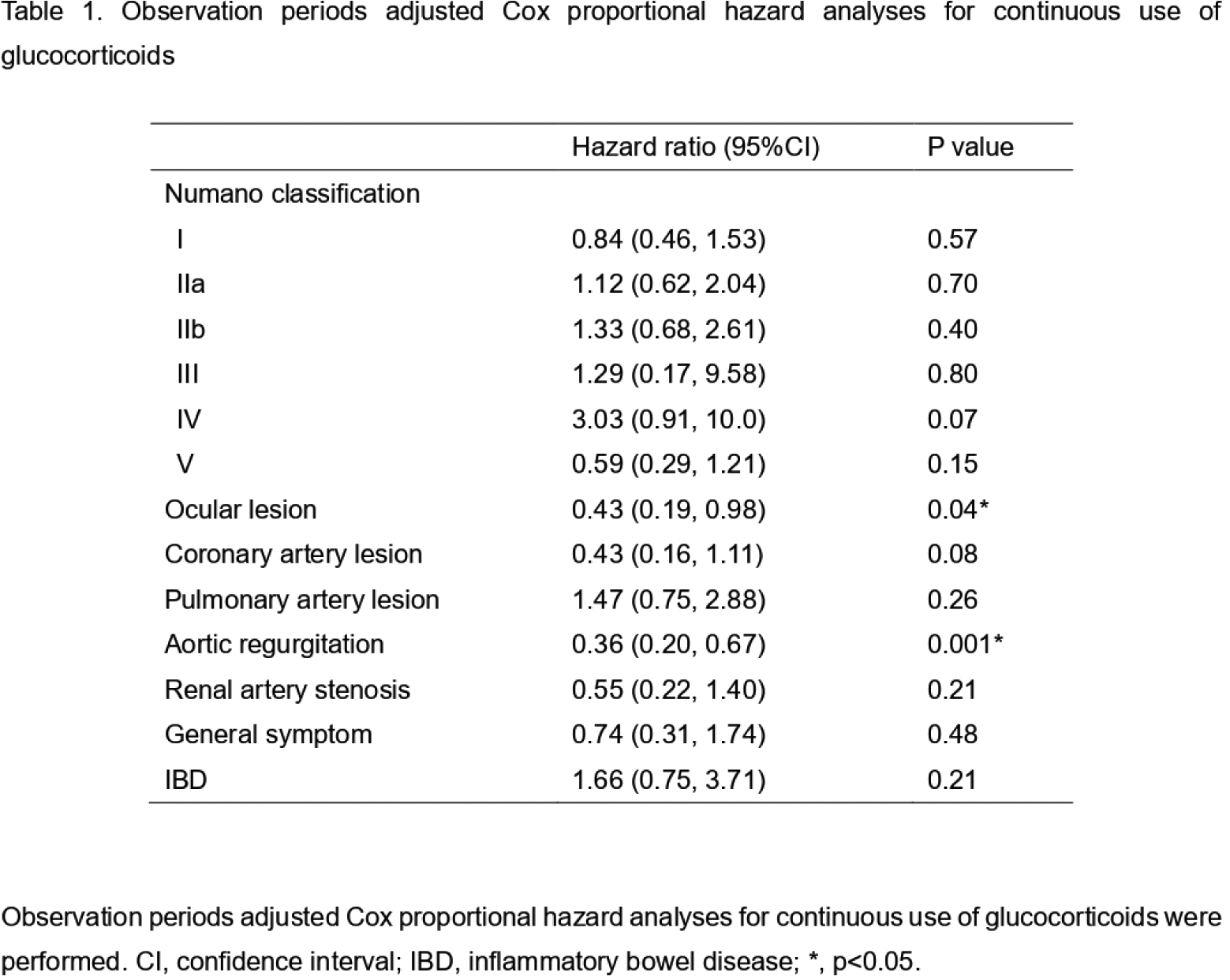
Results: Of the 115 patients (male: n=3, female: n=112) initially registered, 72 patients with a history of GC treatment were eligible for the study, comprising 22 patients with juvenile-onset and 50 patients with adult-onset. The mean age of onset was lower in the juvenile-onset group (15.8±3.6 years) compared to the adult-onset group (32.2±10.1 years). There were no significant differences in sex (100% female in both groups) or observation period (juvenile-onset vs adult-onset: 22.7±13.7 years vs 21.3±13.2 years, p=0.72). Regarding clinical features, the juvenile-onset group showed a significantly lower frequency of aortic regurgitation (27% vs 53%, p=0.04) and a significantly higher frequency of renal artery stenosis (18% vs 4%, p=0.048) (Figure 1A). Based on the Numano classification [2], Type IIa tended to be less frequent (14% vs 28%, p=0.24) and Type V tended to be more frequent (36% vs 16%, p=0.07) in the juvenile-onset group compared to the adult-onset group. When the effect of the juvenile-onset on clinical characteristics was analyzed using logistic regression, the juvenile-onset showed a negative effect on aortic regurgitation (odds ratio: 0.33, 95% confidence interval [CI]: 0.11–0.99, p=0.048). Regarding treatment, no significant differences were observed between the two groups in the maximum prednisolone dose (35.9±15.1 mg vs 35.1±24.6 mg, p=0.33), the usage of GC (100% vs 100%, p=1), aspirin (91% vs 84%, p=0.71), immunosuppressants (55% vs 52%, p=1), and biologic agents (41% vs 26%, p=0.27). In the juvenile-onset group, HLA-B52 (50%) was the most commonly observed allele, followed by HLA-B62 (38%) and HLA-B35 (31%) (Figure 1B). On the other hand, in the adult-onset group, HLA-B52 (73%) was the most common, followed by HLA-B61 (22%) and HLA-B46 (16%). HLA-B52 tended to be more frequently observed in the adult-onset group (juvenile-onset vs adult-onset, 50% vs 73%, p=0.18). HLA-B62 (38% vs 8%, p=0.02) was significantly more frequent in the juvenile-onset group compared to the adult-onset group. A logistic regression analysis demonstrated that HLA-B62 was associated with juvenile-onset, with an odds ratio of 7.08 (95% CI: 1.39–36.0, p=0.02). Of the 72 patients treated with GC, 14 patients subsequently achieved GC-free condition over a period of 13.2±9.0 years of the 26.0±13.9-year observation period. The 30-year cumulative GC-free remission rate was 24%. Only one case among the juvenile-onset group achieved GC-free remission. The cumulative GC-free remission rates were significantly lower in the juvenile-onset group compared to the adult-onset group (juvenile-onset vs adult-onset, 5% vs 32%, p=0.047) (Figure 1C). The observation periods adjusted Cox proportional hazards analysis showed the association between GC-free condition with ocular lesion (hazard ratio [HR]: 0.43, 95%CI: 0.19–0.98, p=0.04), aortic regurgitation (HR: 0.36, 95%CI: 0.20–0.67, p=0.001) (Table 1).
Conclusions: Juvenile-onset Takayasu arteritis has a worse prognosis compared to adult-onset Takayasu arteritis, characterized by distinct differences in vascular lesions and HLA-B profiles. The severe disease may require sustained GC therapy. Because of its retrospective nature, a prospective study is warranted in the future.
REFERENCES: [1] Ruperto N, Ozen S, Pistorio A, et al. Ann Rheum Dis 2010;69:790-7.
[2] Hata A, Noda M, Moriwaki R, et al. Int J Cardiol 1996;54 Suppl:S155-63.
Acknowledgments: NIL.
Disclosure of Interests: HIDEAKI TSUJI speaker fees from Asahi Kasei Pharma Co., Boehringer Ingelheim Japan Co., and Daiichi Sankyo Co. Ltd. outside the work, HT has received research grants from the Japan college of rheumatology, the Shimizu foundation for immunology and neuroscience, Japan Rheumatism Foundation, The Nakatomi Foundation outside the work, Hajime Yoshifuji HY has received consulting fees and honoraria from Janssen, and honoraria from Chugai and AbbVie, outside the work, Tsuneo Sasai: None declared, Mirei Shirakashi: None declared, Ryosuke Hiwa: None declared, Shuji Akizuki: None declared, Ran Nakashima: None declared, Akira Onishi: None declared, Masao Tanaka: None declared, Akio Morinobu: None declared.